

Clinical implementation of intensity modulated proton therapy for thoracic malignancies
- PMID: 25260491
- PMCID: PMC4252731
- DOI: 10.1016/j.ijrobp.2014.07.045
Clinical implementation of intensity modulated proton therapy for thoracic malignancies
Abstract
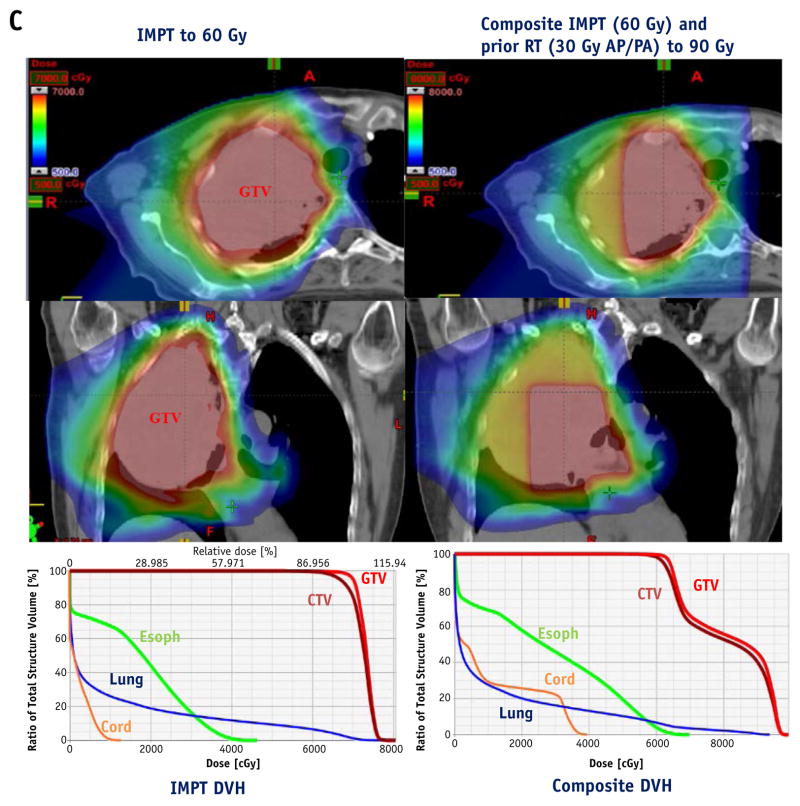
Purpose: Intensity modulated proton therapy (IMPT) can improve dose conformality and better spare normal tissue over passive scattering techniques, but range uncertainties complicate its use, particularly for moving targets. We report our early experience with IMPT for thoracic malignancies in terms of motion analysis and management, plan optimization and robustness, and quality assurance.
Methods and materials: Thirty-four consecutive patients with lung/mediastinal cancers received IMPT to a median 66 Gy(relative biological equivalence [RBE]). All patients were able to undergo definitive radiation therapy. IMPT was used when the treating physician judged that IMPT conferred a dosimetric advantage; all patients had minimal tumor motion (<5 mm) and underwent individualized tumor-motion dose-uncertainty analysis and 4-dimensional (4D) computed tomographic (CT)-based treatment simulation and motion analysis. Plan robustness was optimized by using a worst-case scenario method. All patients had 4D CT repeated simulation during treatment.
Results: IMPT produced lower mean lung dose (MLD), lung V5 and V20, heart V40, and esophageal V60 than did IMRT (P<.05) and lower MLD, lung V20, and esophageal V60 than did passive scattering proton therapy (PSPT) (P<.05). D5 to the gross tumor volume and clinical target volume was higher with IMPT than with intensity modulated radiation therapy or PSPT (P<.05). All cases were analyzed for beam-angle-specific motion, water-equivalent thickness, and robustness. Beam angles were chosen to minimize the effect of respiratory motion and avoid previously treated regions, and the maximum deviation from the nominal dose-volume histogram values was kept at <5% for the target dose and met the normal tissue constraints under a worst-case scenario. Patient-specific quality assurance measurements showed that a median 99% (range, 95% to 100%) of the pixels met the 3% dose/3 mm distance criteria for the γ index. Adaptive replanning was used for 9 patients (26.5%).
Conclusions: IMPT using 4D CT-based planning, motion management, and optimization was implemented successfully and met our quality assurance parameters for treating challenging thoracic cancers.
Copyright © 2014 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest: none.
Figures





References
-
- Chang JY, Zhang X, Wang X, et al. Significant reduction of normal tissue dose by proton radiotherapy compared with three-dimensional conformal or intensity-modulated radiation therapy in stage I or stage III non-small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2006;65:1087–1096. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
