

Surgical and anaesthetic capacity of hospitals in Malawi: key insights
- PMID: 25261799
- PMCID: PMC4559113
- DOI: 10.1093/heapol/czu102
Surgical and anaesthetic capacity of hospitals in Malawi: key insights
Abstract
Background: Surgery is increasingly recognized as an important driver for health systems strengthening, especially in developing countries. To facilitate quality improvement initiatives, baseline knowledge of capacity for surgical, anaesthetic, emergency and obstetric care is critical. In partnership with the Malawi Ministry of Health, we quantified government hospitals' surgical capacity through workforce, infrastructure and health service delivery components.
Methods: From November 2012 to January 2013, we surveyed district and mission hospital administrators and clinical staff onsite using a modified version of the Personnel, Infrastructure, Procedures, Equipment and Supplies (PIPES) tool from Surgeons OverSeas. We calculated percentage of facilities demonstrating adequacy of the assessed components, surgical case rates, operating theatre density and surgical workforce density.
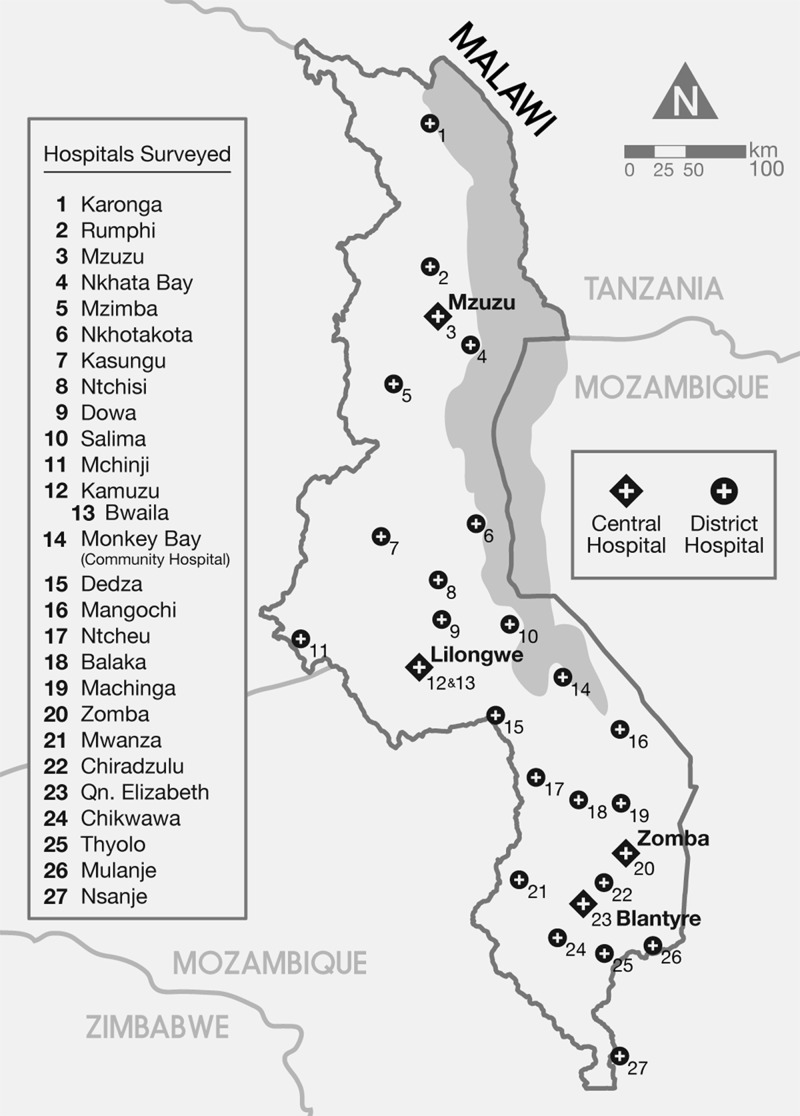
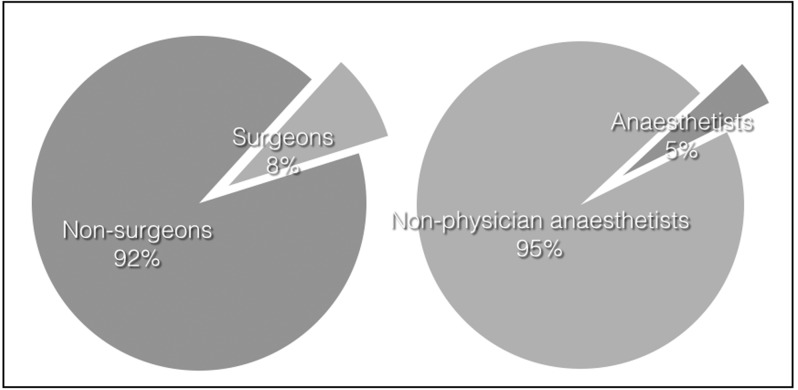
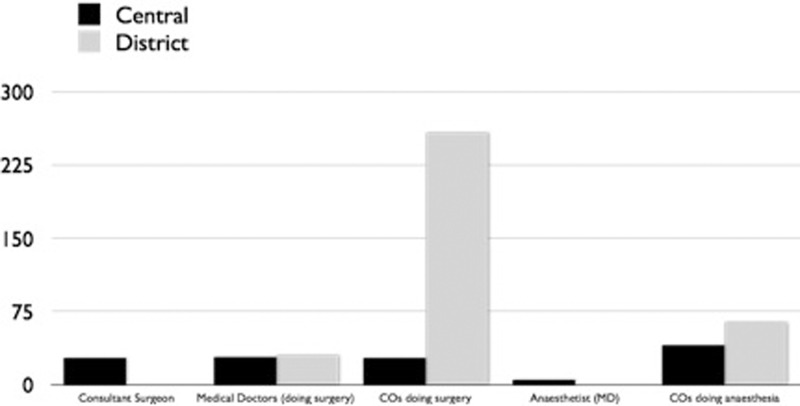
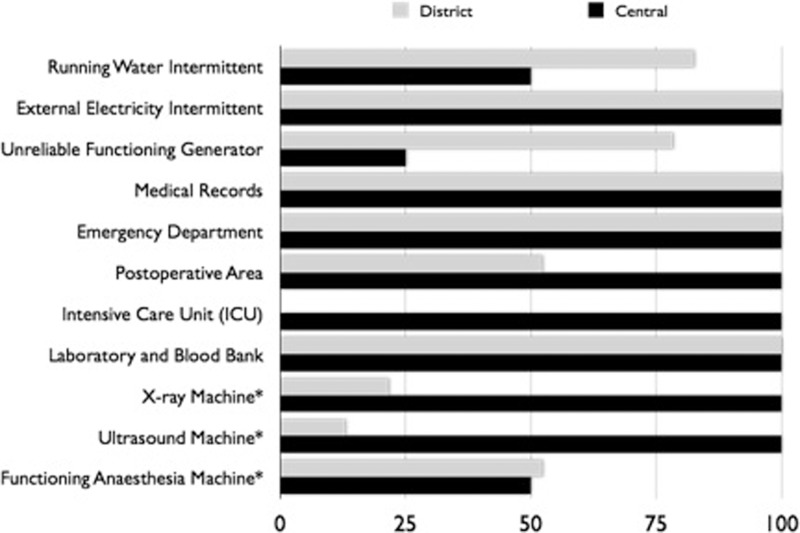
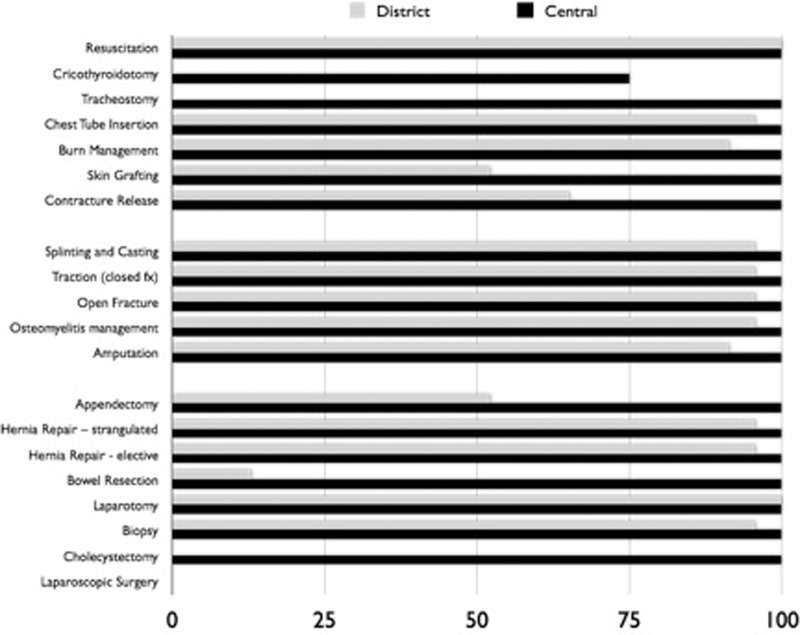
Results: Twenty-seven government hospitals were surveyed (90% of the district hospitals, all central hospitals). Of the surgical workforce surveyed (n = 370), 92.7% were non-surgeons and 77% were clinical officers (COs). Of the 109 anaesthesia providers, 95.4% were non-physician anaesthetists (anaesthesia COs or ACOs). Non-surgeons and ACOs were the only providers of surgical services and anaesthetic services in 85% and 88.9% of hospitals, respectively. No specialists served the district hospitals. All of the hospitals experienced periods without external electricity. Most did not always have a functioning generator (78.3% district, 25% central) or running water (82.6%, 50%). None of the district hospitals had an Intensive Care Unit (ICU). Cricothyroidotomy, bowel resection and cholecystectomy were not done in over two-thirds of hospitals. Every hospital provided general anaesthesia but some did not always have a functioning anaesthesia machine (52.2%, 50%). Surgical rate, operating theatre density and surgical workforce density per 100 000 population was 289.48-747.38 procedures, 0.98 and 5.41 and 3.68 surgical providers, respectively.
Conclusion: COs form the backbone of Malawi's surgical and anaesthetic workforce and should be supported with improvements in infrastructure as well as training and mentorship by specialist surgeons and anaesthetists.
Keywords: Anaesthesia; Malawi; clinical officers; global health; global surgery; surgery; surgical burden; surgical capacity; surgical care.
Published by Oxford University Press in association with The London School of Hygiene and Tropical Medicine © The Author 2014; all rights reserved.
Figures
References
-
- American College of Surgeons (ACS) 2010. Health Policy Research Institute. The Supply of Surgeons in the United States: Mapping the 50 States. http://mcacs.org/files/2010/Massachusetts-Surgeon-Map.pdf, accessed 23 April 2014.
-
- Central Intelligence Agency (CIA) The World Factbook. 2013–14. https://www.cia.gov/library/publications/the-world-factbook/index.html, accessed 19 June 2013.
-
- Debas HT, et al. Surgery. In: Jamison DT, et al., editors. Disease Control Priorities in Developing Countries. 2nd. New York: Oxford University Press; 2006. pp. 1245–60.
-
- The Demographic and Health Surveys (DHS) 2014. http://www.dhsprogram.com/pubs/pdf/SPAQ5/Service_Readiness_Indicators_04..., accessed 23 April 2014.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
