

Intensive postoperative glucose control reduces the surgical site infection rates in gynecologic oncology patients
- PMID: 25263249
- PMCID: PMC4755696
- DOI: 10.1016/j.ygyno.2014.09.013
Intensive postoperative glucose control reduces the surgical site infection rates in gynecologic oncology patients
Abstract
Objective: SSI rates after gynecologic oncology surgery vary from 5% to 35%, but are up to 45% in patients with diabetes mellitus (DM). Strict postoperative glucose control by insulin infusion has been shown to lower morbidity, but not specifically SSI rates. Our project studied continuous postoperative insulin infusion for 24h for gynecologic oncology patients with DM and hyperglycemia with a target blood glucose of <139 mL/dL and a primary outcome of the protocol's impact on SSI rates.
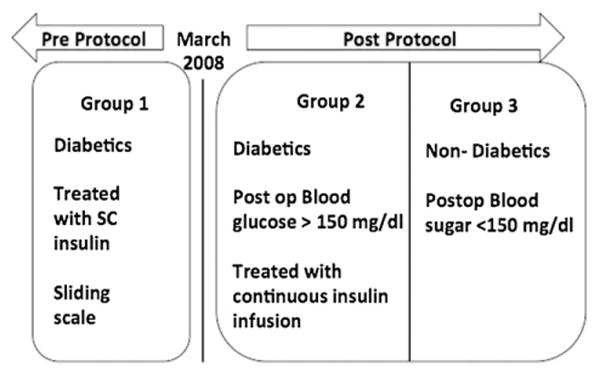
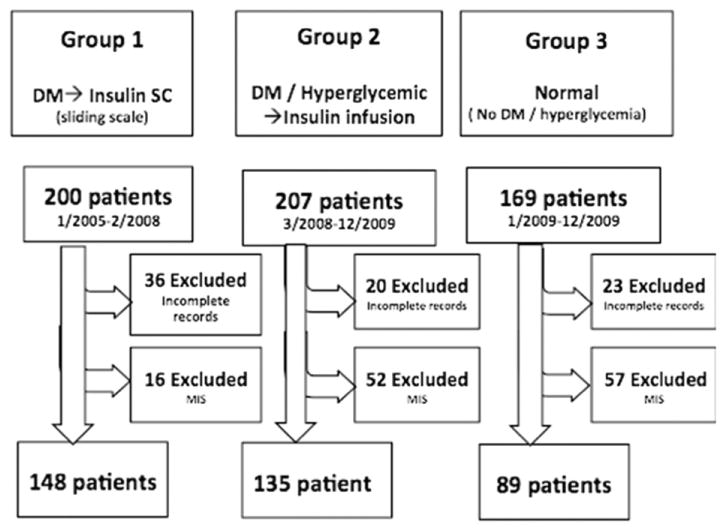
Methods: We compared SSI rates retrospectively among three groups. Group 1 was composed of patients with DM whose blood glucose was controlled with intermittent subcutaneous insulin injections. Group 2 was composed of patients with DM and postoperative hyperglycemia whose blood glucose was controlled by insulin infusion. Group 3 was composed of patients with neither DM nor hyperglycemia. We controlled for all relevant factors associated with SSI.
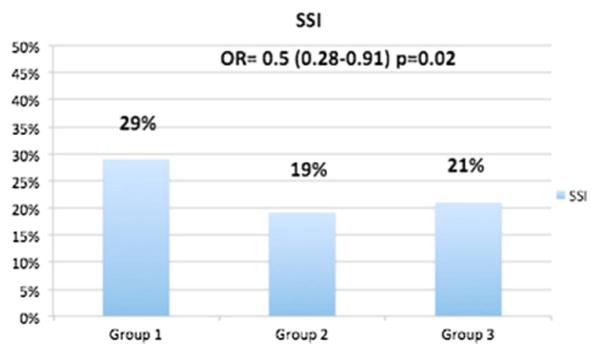
Results: We studied a total of 372 patients. Patients in Group 2 had an SSI rate of 26/135 (19%), similar to patients in Group 3 whose rate was 19/89 (21%). Both were significantly lower than the SSI rate (43/148, 29%) of patients in Group 1. This reduction of 35% is significant (p = 0.02). Multivariate analysis showed an odd ratio = 0.5 (0.28-0.91) in reducing SSI rates after instituting this protocol.
Conclusions: Initiating intensive glycemic control for 24h after gynecologic oncology surgery in patients with DM and postoperative hyperglycemia lowers the SSI rate by 35% (OR = 0.5) compared to patients receiving intermittent sliding scale insulin and to a rate equivalent to non-diabetics.
Keywords: Diabetes mellitus; Gynecologic oncology surgery; Intensive glycemic control; Post operative morbidity; Surgical outcome; Surgical site infection.
Copyright © 2014. Published by Elsevier Inc.
Conflict of interest statement
Figures
References
-
- Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999. Centers for Disease Control and Prevention (CDC) Hospital Infection Control Practices Advisory Committee. Am J Infect Control. 1999;27:97–132. quiz 3–4; discussion 96. - PubMed
-
- Nugent EK, Hoff JT, Gao F, Massad LS, Case A, Zighelboim I, et al. Wound complications after gynecologic cancer surgery. Gynecol Oncol. 2011;121:347–52. - PubMed
-
- de Lissovoy G, Fraeman K, Hutchins V, Murphy D, Song D, Vaughn BB. Surgical site infection: incidence and impact on hospital utilization and treatment costs. Am J Infect Control. 2009;37:387–97. - PubMed
-
- Ata A, Valerian BT, Lee EC, Bestle SL, Elmendorf SL, Stain SC. The effect of diabetes mellitus on surgical site infections after colorectal and noncolorectal general surgical operations. Am Surg. 2010;76:697–702. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
