

Variation among United States hospitals in inpatient mortality for cirrhosis
- PMID: 25264271
- PMCID: PMC4333025
- DOI: 10.1016/j.cgh.2014.09.038
Variation among United States hospitals in inpatient mortality for cirrhosis
Abstract
Background & aims: Little is known about geographic variations in health care for patients with cirrhosis. We studied geographic and hospital-level variations in care of patients with cirrhosis in the United States by using inpatient mortality as an outcome for comparing hospitals. We also aimed to identify features of patients and hospitals associated with lower mortality.
Methods: We used the 2009 U.S. Nationwide Inpatient Sample to identify patients with cirrhosis, which were based on the International Classification of Diseases, 9th Revision-Clinical Modification diagnosis codes for cirrhosis or 1 of its complications (ascites, hepatorenal syndrome, upper gastrointestinal bleeding, portal hypertension, or hepatic encephalopathy). Multilevel modeling was performed to measure variance among hospitals.
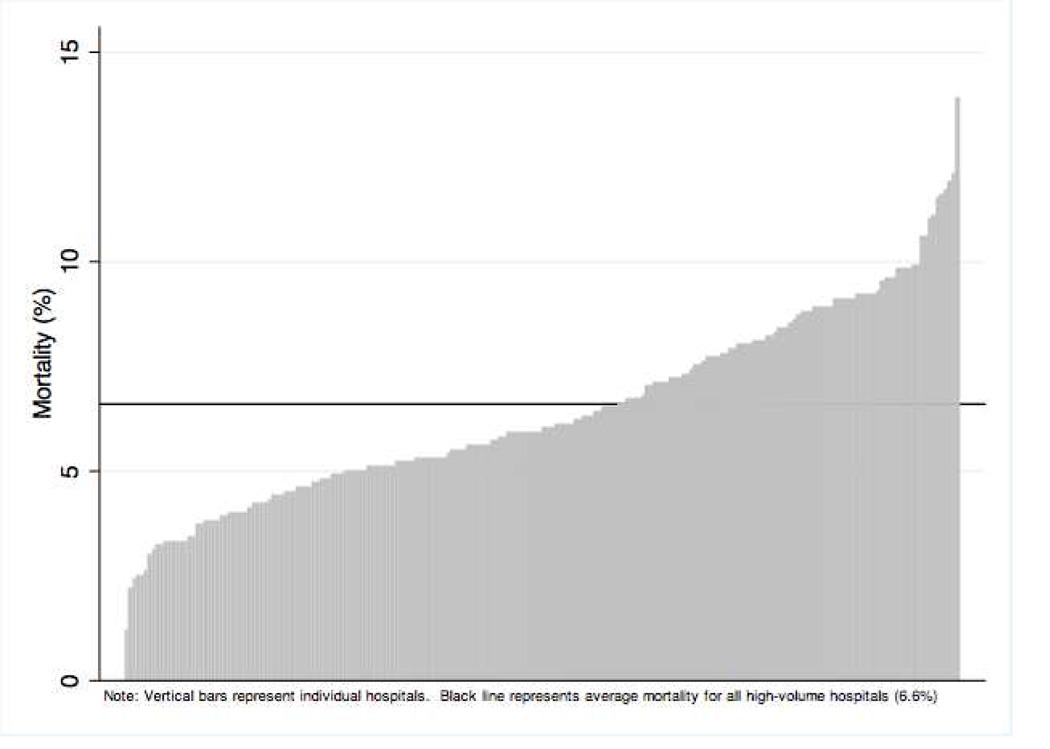
Results: There were 102,155 admissions for cirrhosis in 2009, compared with 74,417 in 2003. Overall inpatient mortality was 6.6%. On multivariable-adjusted logistic regression, patients hospitalized in the Midwest had the lowest odds ratio (OR) of inpatient mortality (OR, 0.54; P < .001). Patients who were transferred from other hospitals (OR, 1.49; P < .001) or had hepatic encephalopathy (OR, 1.28; P < .001), upper gastrointestinal bleeding (OR, 1.74; P < .001), or alcoholic liver disease (OR, 1.23; P = .03) had higher odds of inpatient mortality than patients without these features. Those who received liver transplants had substantially lower odds of inpatient mortality (OR, 0.21; P < .001). Multilevel modeling showed that 4% of the variation in mortality could be accounted for at the hospital level (P < .001). Adjusted mortality among hospitals ranged from 1.2% to 14.2%.
Conclusions: Inpatient cirrhosis mortality varies considerably among U.S. hospitals. Further research is needed to identify hospital-level and provider-level practices that could be modified to improve outcomes.
Keywords: Chronic Liver Disease; NIS; Regional Variation; Survival.
Copyright © 2015 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
JLM- none
CRR-none
AKM-none
MLV-none
Figures
References
-
- Ghaferi AA, Birkmeyer JD, Dimick JB. Variation in hospital mortality associated with inpatient surgery. N. Engl. J. Med. 2009;361:1368–1375. - PubMed
-
- Newhouse JP, Garber AM. Geographic variation in Medicare services. N. Engl. J. Med. 2013;368:1465–1468. - PubMed
-
- Newhouse JP, Garber A, Graham RP. Interim Report of the Committee on Geographic Variation in Health Care Spending and Promotion of High-Value Health Care: Preliminary Committee. Washington, DC: National Academies Press; 2013. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
