

Electroencephalographic variation during end maintenance and emergence from surgical anesthesia
- PMID: 25264892
- PMCID: PMC4180055
- DOI: 10.1371/journal.pone.0106291
Electroencephalographic variation during end maintenance and emergence from surgical anesthesia
Abstract
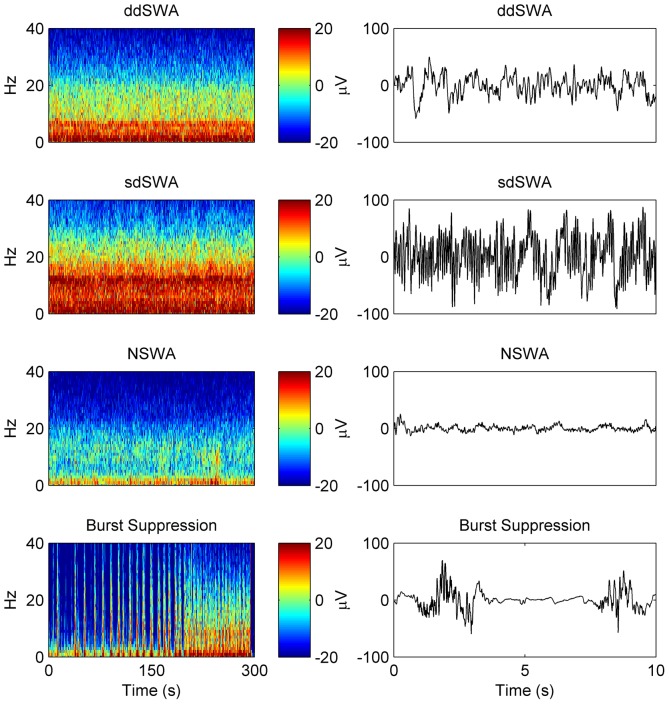
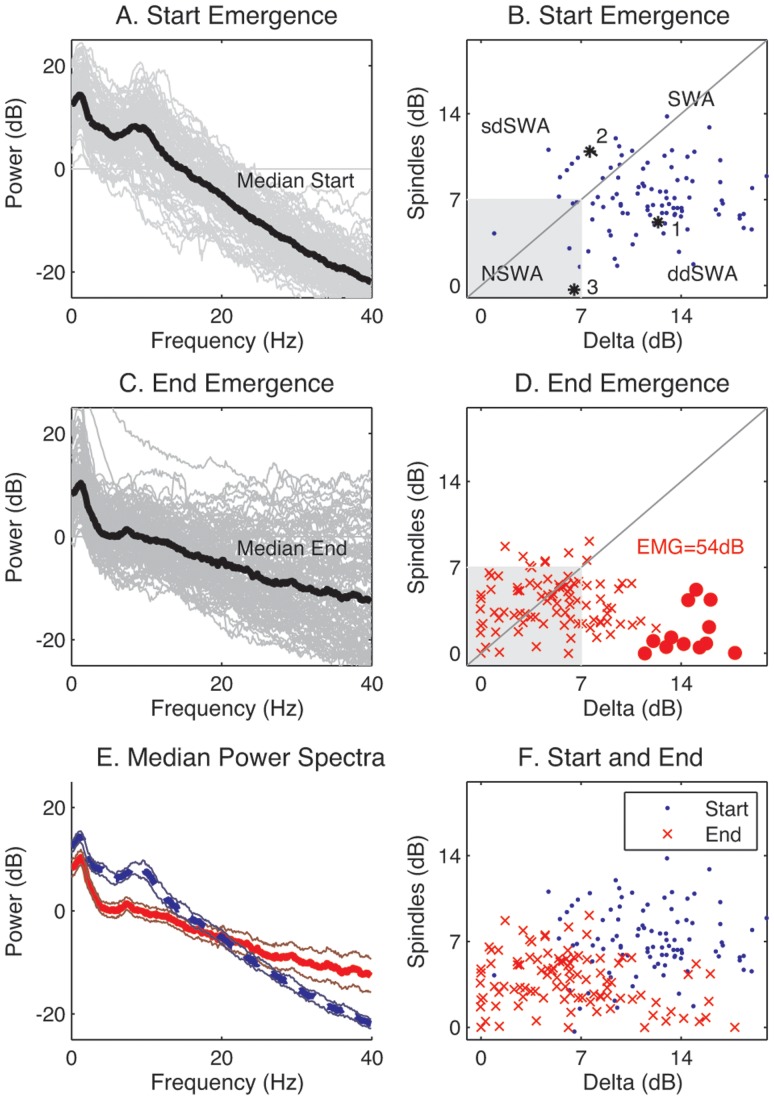
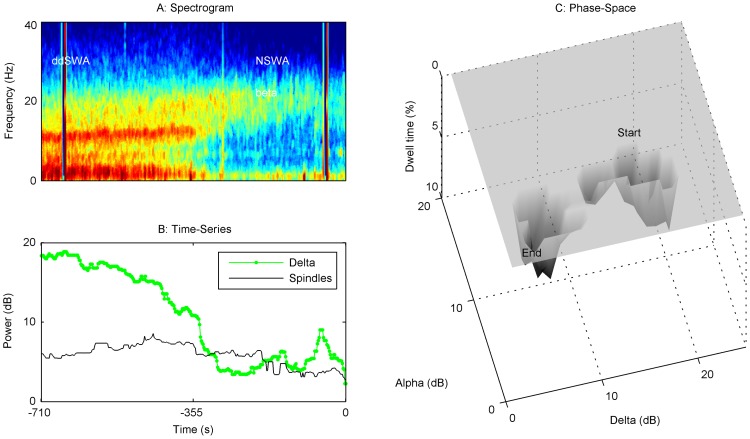
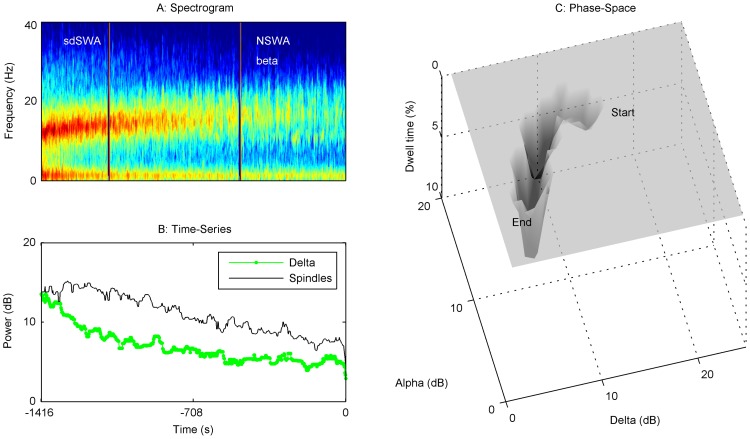
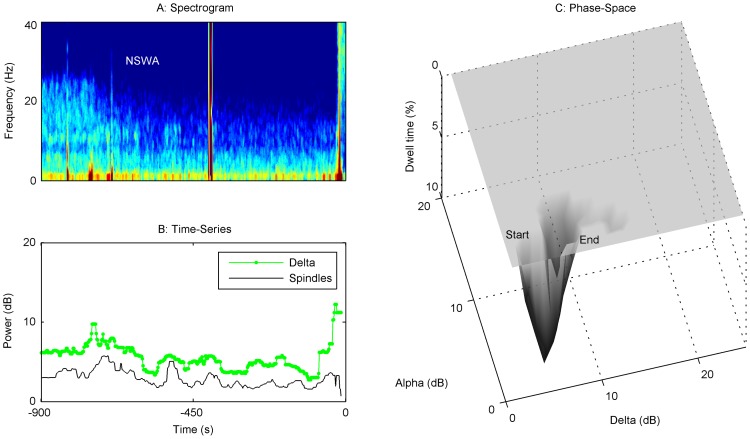
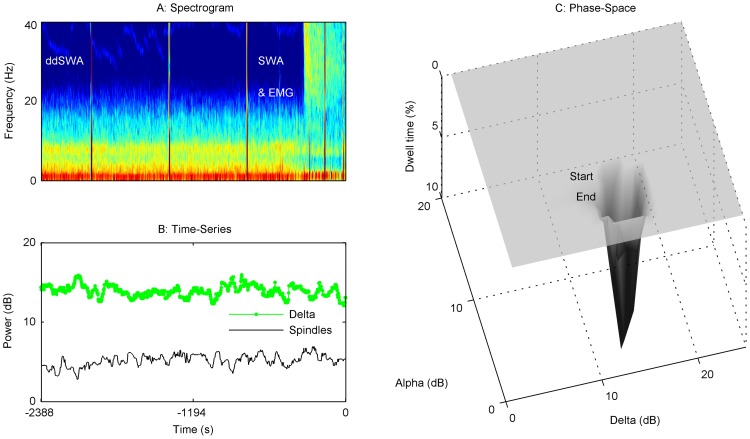
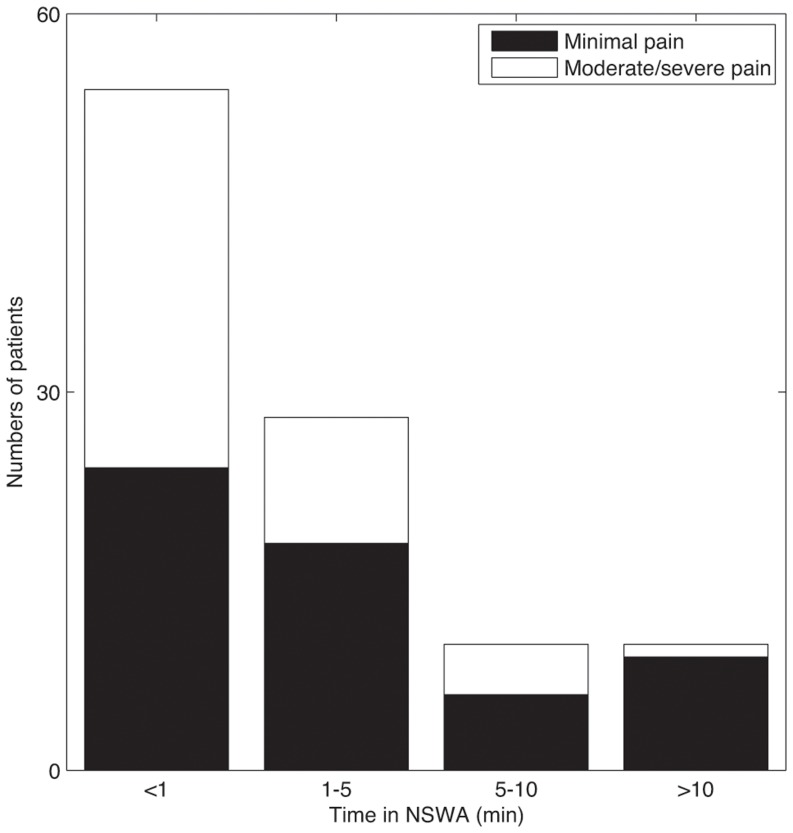
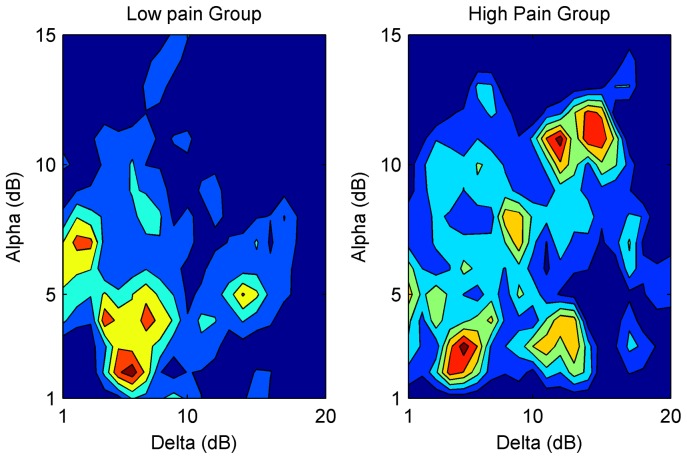
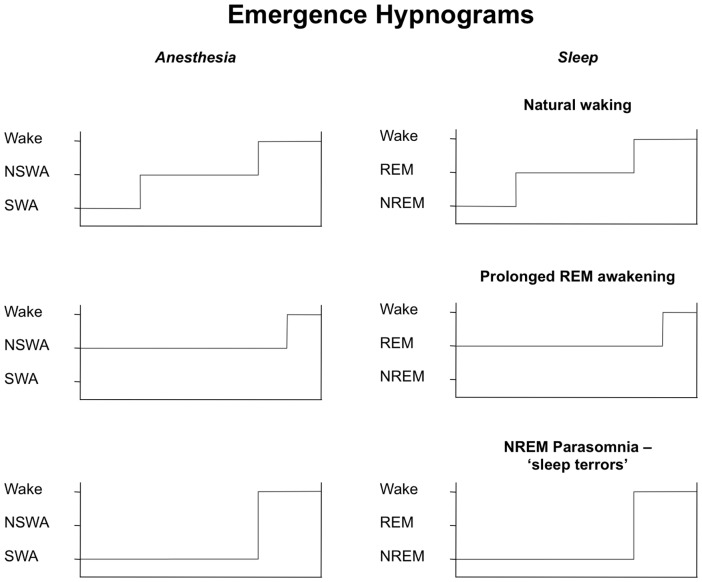
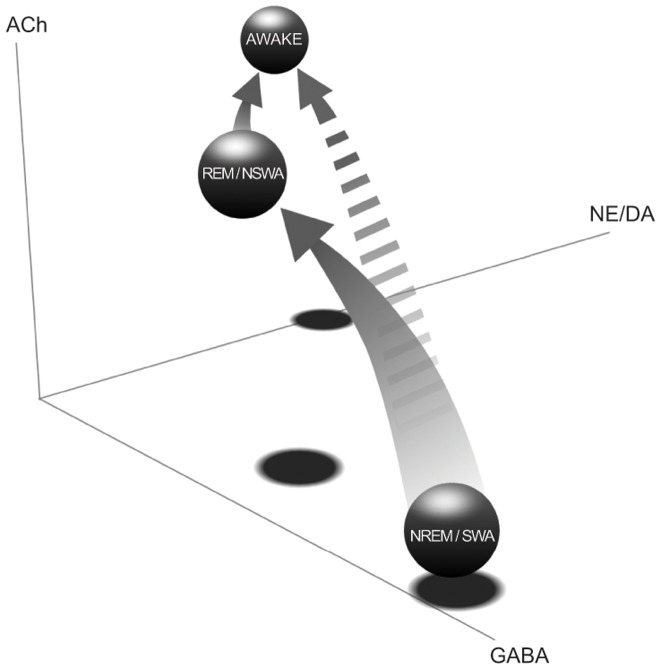
The re-establishment of conscious awareness after discontinuing general anesthesia has often been assumed to be the inverse of loss of consciousness. This is despite the obvious asymmetry in the initiation and termination of natural sleep. In order to characterize the restoration of consciousness after surgery, we recorded frontal electroencephalograph (EEG) from 100 patients in the operating room during maintenance and emergence from general anesthesia. We have defined, for the first time, 4 steady-state patterns of anesthetic maintenance based on the relative EEG power in the slow-wave (<14 Hz) frequency bands that dominate sleep and anesthesia. Unlike single-drug experiments performed in healthy volunteers, we found that surgical patients exhibited greater electroencephalographic heterogeneity while re-establishing conscious awareness after drug discontinuation. Moreover, these emergence patterns could be broadly grouped according to the duration and rapidity of transitions amongst these slow-wave dominated brain states that precede awakening. Most patients progressed gradually from a pattern characterized by strong peaks of delta (0.5-4 Hz) and alpha/spindle (8-14 Hz) power ('Slow-Wave Anesthesia') to a state marked by low delta-spindle power ('Non Slow-Wave Anesthesia') before awakening. However, 31% of patients transitioned abruptly from Slow-Wave Anesthesia to waking; they were also more likely to express pain in the post-operative period. Our results, based on sleep-staging classification, provide the first systematized nomenclature for tracking brain states under general anesthesia from maintenance to emergence, and suggest that these transitions may correlate with post-operative outcomes such as pain.
Conflict of interest statement
Figures
References
-
- Courtin RF, Bickford RG, Faulconer A Jr (1950) The classification and significance of electro-encephalographic patterns produced by nitrous oxide-ether anesthesia during surgical operations. Proc Staff Meet Mayo Clin 25: 197–206. - PubMed
-
- Kiersey DK, Bickford RG, Faulconer A Jr (1951) Electro-encephalographic patterns produced by thiopental sodium during surgical operations; description and classification. Br J Anaesth 23: 141–152. - PubMed
-
- Clark DL, Rosner BS (1973) Neurophysiologic effects of general anesthetics. I. The electroencephalogram and sensory evoked responses in man. Anesthesiology 38: 564–582. - PubMed
-
- Dement W, Kleitman N (1957) Cyclic variations in EEG during sleep and their relation to eye movements, body motility, and dreaming. Electroencephalogr Clin Neurophysiol 9: 673–690. - PubMed
-
- Rechtschaffen A, Kales A (1968) A manual of standardized terminology, techniques, and scoring system for sleep stages of human subjects. University of California, Los Angeles: Brain Information Service/Brain Research Institute.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
