

Spatial and temporal epidemiology of clinical malaria in Cambodia 2004-2013
- PMID: 25266007
- PMCID: PMC4531392
- DOI: 10.1186/1475-2875-13-385
Spatial and temporal epidemiology of clinical malaria in Cambodia 2004-2013
Abstract
Background: Artemisinin-resistant Plasmodium falciparum malaria has recently been identified on the Thailand-Cambodia border and more recently in parts of Thailand, Myanmar and Vietnam. There is concern that if this resistance were to spread, it would severely hamper malaria control and elimination efforts worldwide. Efforts are currently underway to intensify malaria control activities and ultimately eliminate malaria from Cambodia. To support these efforts, it is crucial to have a detailed picture of disease burden and its major determinants over time.
Methods: An analysis of spatial and temporal data on clinical malaria in Cambodia collected by the National Centre for Parasitology, Entomology and Malaria Control (CNM) and the Department of Planning and Health Information, Ministry of Health Cambodia from 2004 to 2013 is presented.
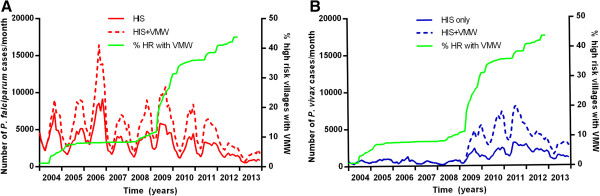
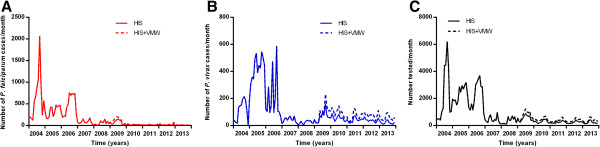
Results: There has been a marked decrease of 81% in annual cases due to P. falciparum since 2009 coinciding with a rapid scale-up in village malaria workers (VMWs) and insecticide-treated bed nets (ITNs). Concurrently, the number of cases with Plasmodium vivax has greatly increased. It is estimated that there were around 112,000 total cases in 2012, 2.8 times greater than the WHO estimate for that year, and 68,000 in 2013 (an annual parasite incidence (API) of 4.6/1000). With the scale-up of VMWs, numbers of patients presenting to government facilities did not fall and it appears likely that those who saw VMWs had previously accessed healthcare in the private sector. Malaria mortality has decreased, particularly in areas with VMWs. There has been a marked decrease in cases in parts of western Cambodia, especially in Pailin and Battambang Provinces. In the northeast, the fall in malaria burden has been more modest, this area having the highest API in 2013.
Conclusion: The clinical burden of falciparum malaria in most areas of Cambodia has greatly decreased from 2009 to 2013, associated with roll-out of ITNs and VMWs. Numbers of cases with P. vivax have increased. Possible reasons for these trends are discussed and areas requiring further study are highlighted. Although malaria surveillance data are prone to collection bias and tend to underestimate disease burden, the finding of similar trends in two independent datasets in this study greatly increased the robustness of the findings.
Figures













References
-
- World Health Organization . Global Partnership to Roll Back Malaria: Global plan for artemisinin resistance containment (GPARC) Geneva: World Health Organization; 2011.
-
- Phyo AP, Nkhoma S, Stepniewska K, Ashley EA, Nair S, McGready R, ler Moo C, Al-Saai S, Dondorp AM, Lwin KM, Singhasivanon P, Day NP, White NJ, Anderson TJ, Nosten F. Emergence of artemisinin-resistant malaria on the western border of Thailand: a longitudinal study. Lancet. 2012;379:1960–1966. doi: 10.1016/S0140-6736(12)60484-X. - DOI - PMC - PubMed
-
- Kyaw MP, Nyunt MH, Chit K, Aye MM, Aye KH, Aye MM, Lindegardh N, Tarning J, Imwong M, Jacob CG, Rasmussen C, Perin J, Ringwald P, Nyunt MM. Reduced susceptibility of Plasmodium falciparum to artesunate in southern Myanmar. PLoS One. 2013;8:e57689. doi: 10.1371/journal.pone.0057689. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
