

Using CD4 percentage and age to optimize pediatric antiretroviral therapy initiation
- PMID: 25266426
- PMCID: PMC4179097
- DOI: 10.1542/peds.2014-0527
Using CD4 percentage and age to optimize pediatric antiretroviral therapy initiation
Abstract
Background: Quantifying pediatric immunologic recovery by highly active antiretroviral therapy (HAART) initiation at different CD4 percentage (CD4%) and age thresholds may inform decisions about timing of treatment initiation.
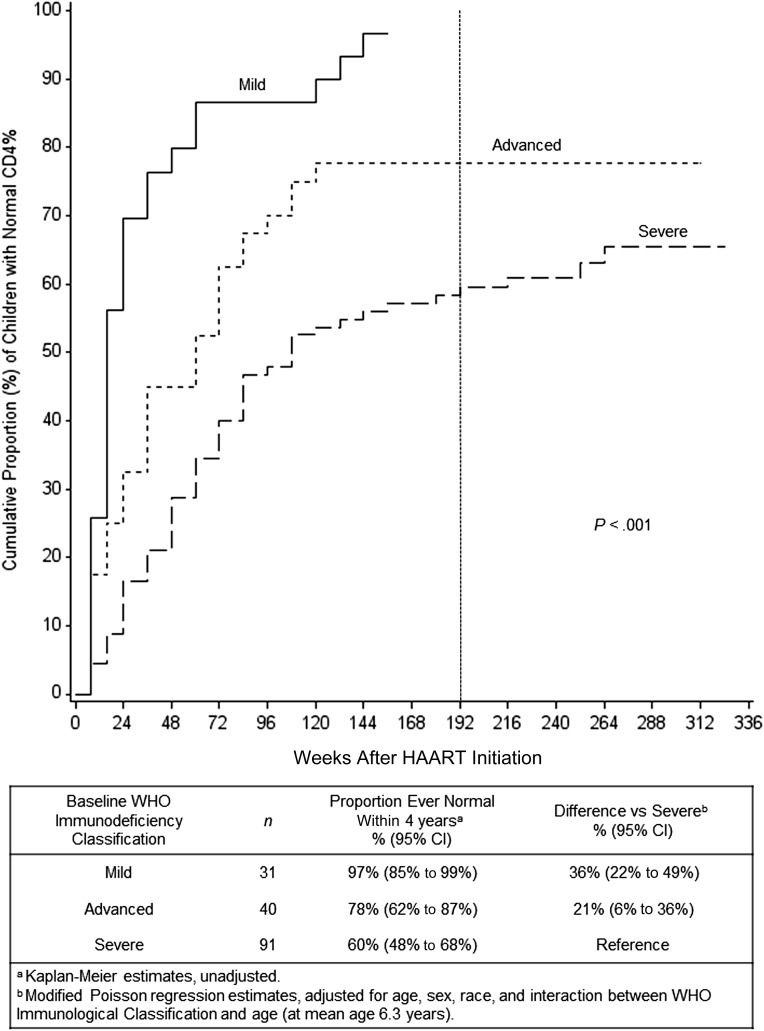
Methods: HIV-1-infected, HAART-naive children in Europe and the Americas were followed from 2002 through 2009 in PENPACT-1. Data from 162 vertically infected children, with at least World Health Organization "mild" immunosuppression and CD4% <10th percentile, were analyzed for improvement to a normal CD4% (≥10th percentile) within 4 years after HAART initiation. Data from 209 vertically infected children, regardless of immune status, were analyzed for CD4% outcomes at 4 years and viral failure within 4 years.
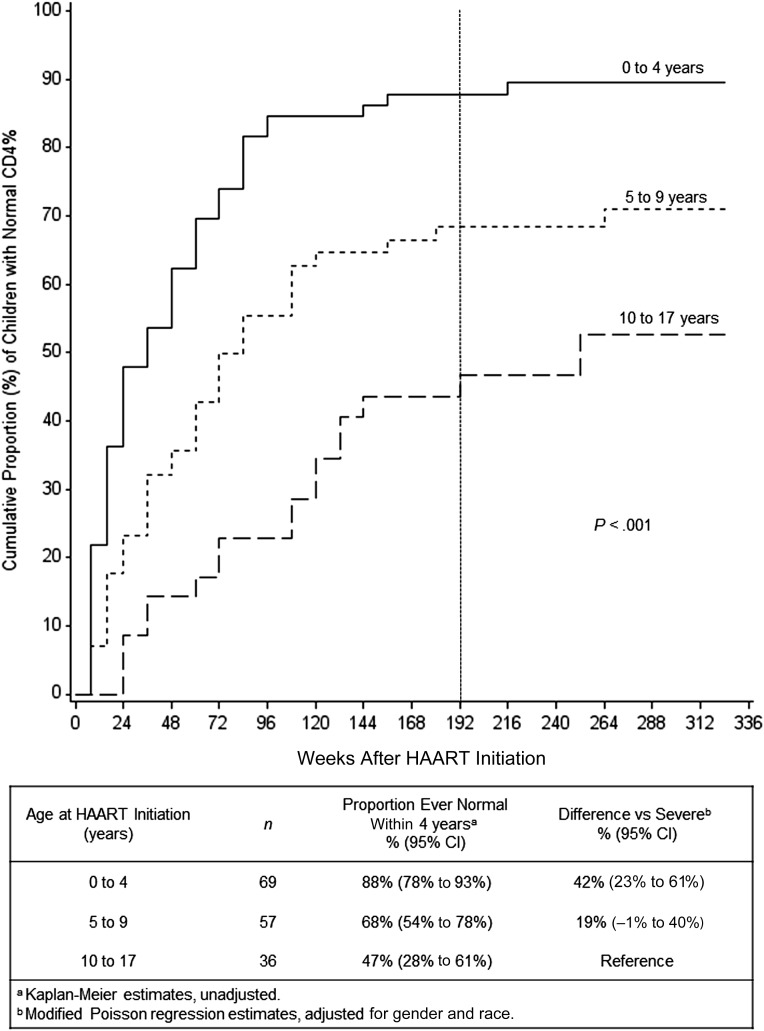
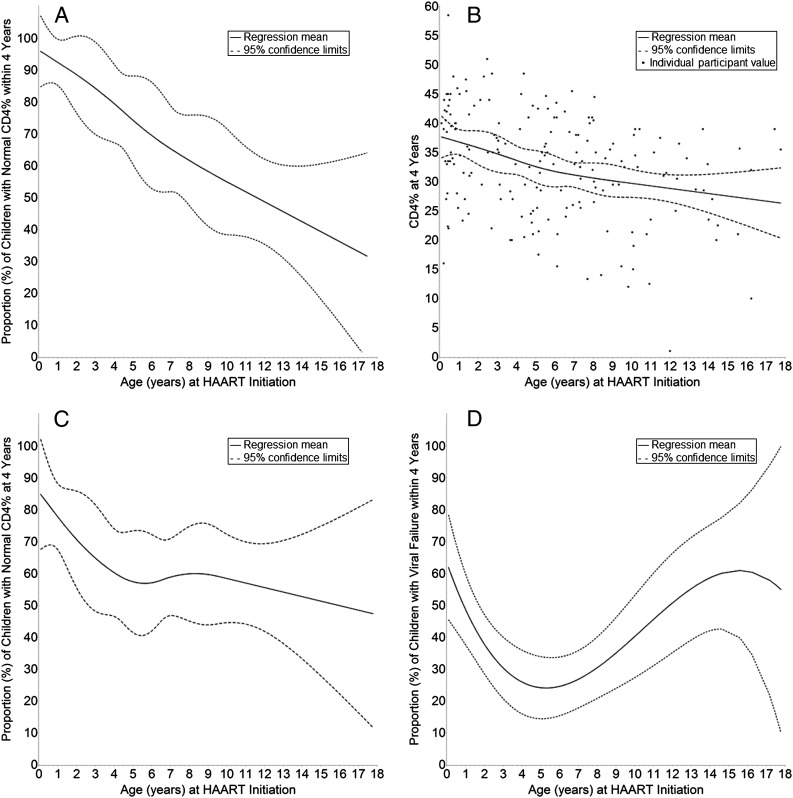
Results: Seventy-two percent of baseline immunosuppressed children recovered to normal within 4 years. Compared with "severe" immunosuppression, more children with "mild" immunosuppression (difference 36%, 95% confidence interval [CI]: 22% to 49%) or "advanced" immunosuppression (difference 20.8%, 95% CI: 5.8% to 35.9%) recovered a normal CD4%. For each 5-year increase in baseline age, the proportion of children achieving a normal CD4% declined by 19% (95% CI: 11% to 27%). Combining baseline CD4% and age effects resulted in >90% recovery when initiating HAART with "mild" immunosuppression at any age or "advanced" immunosuppression at age <3 years. Baseline CD4% effects became greater with increasing age (P = .02). At 4 years, most immunologic benefits were still significant but diminished. Viral failure was highest in infancy (56%) and adolescence (63%).
Conclusions: Initiating HAART at higher CD4% and younger ages maximizes potential for immunologic recovery. Guidelines should weigh immunologic benefits against long-term risks.
Keywords: HIV; child; immunologic; reconstitution; treatment failure.
Copyright © 2014 by the American Academy of Pediatrics.
Figures
References
-
- Joint United Nations Programme on HIV/AIDS. Global Report: UNAIDS report on the global AIDS epidemic 2013. Geneva, Switzerland: WHO Library Cataloguing-in-Publication Data; 2013. Available at: http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiolo.... Accessed October 14, 2013
-
- Patel K, Hernán MA, Williams PL, et al. Pediatric AIDS Clinical Trials Group 219/219C Study Team . Long-term effectiveness of highly active antiretroviral therapy on the survival of children and adolescents with HIV infection: a 10-year follow-up study. Clin Infect Dis. 2008;46(4):507–515 - PubMed
-
- Dunn D, HIV Paediatric Prognostic Markers Collaborative Study Group . Short-term risk of disease progression in HIV-1-infected children receiving no antiretroviral therapy or zidovudine monotherapy: a meta-analysis. Lancet. 2003;362(9396):1605–1611 - PubMed
-
- Resino S, Micheloud D, Larrú B, et al. Spanish Group of Paediatric HIV Infection . Immunological recovery and metabolic disorders in severe immunodeficiency HIV type 1-infected children on highly active antiretroviral therapy. AIDS Res Hum Retroviruses. 2008;24(12):1477–1484 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- G1001190/MRC_/Medical Research Council/United Kingdom
- T32 HD043029/HD/NICHD NIH HHS/United States
- HHSN267200800001G/DK/NIDDK NIH HHS/United States
- U01 AI068632/AI/NIAID NIH HHS/United States
- UM1 AI068632/AI/NIAID NIH HHS/United States
- MC_U122886353/MRC_/Medical Research Council/United Kingdom
- U01 AI068616/AI/NIAID NIH HHS/United States
- HHSN267200800001C/HD/NICHD NIH HHS/United States
- U01 AI041110/AI/NIAID NIH HHS/United States
- UL1 RR025014/RR/NCRR NIH HHS/United States
- UM1 AI068616/AI/NIAID NIH HHS/United States
- N01-DK-9-001/HHSN267200800001C/DK/NIDDK NIH HHS/United States
- T32 HD060558/HD/NICHD NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- AI068632/AI/NIAID NIH HHS/United States
- UL1 TR002319/TR/NCATS NIH HHS/United States
- 1 U01 AI068616/AI/NIAID NIH HHS/United States
- 5 U01 AI41110/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
