

Vascular access type, inflammatory markers, and mortality in incident hemodialysis patients: the Choices for Healthy Outcomes in Caring for End-Stage Renal Disease (CHOICE) Study
- PMID: 25266479
- PMCID: PMC4265216
- DOI: 10.1053/j.ajkd.2014.07.010
Vascular access type, inflammatory markers, and mortality in incident hemodialysis patients: the Choices for Healthy Outcomes in Caring for End-Stage Renal Disease (CHOICE) Study
Abstract
Background: Few reports have shown an association between access type and inflammatory marker levels in a longitudinal cohort. We investigated the role of access type on serial levels of inflammatory markers and the role of inflammatory markers in mediating the association of access type and risk of mortality in a prospective study of incident dialysis patients.
Study design: Cohort study, post hoc analysis of the CHOICE (Choices for Healthy Outcomes in Caring for ESRD) Study.
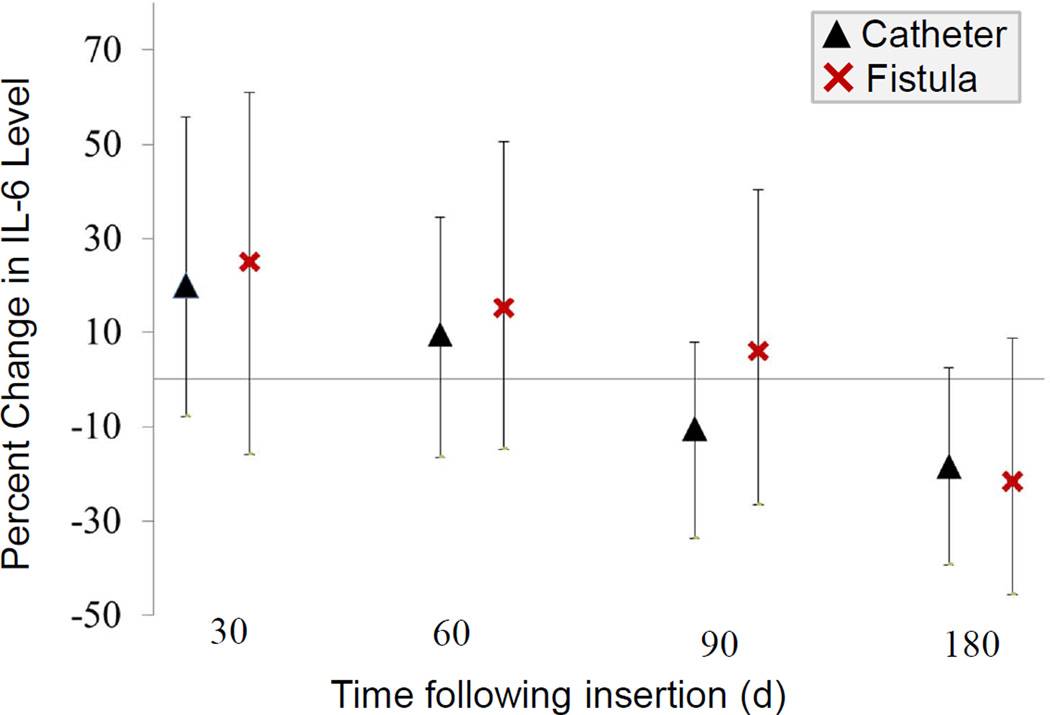
Setting & participants: In 583 participants, inflammation was assessed by measuring serum C-reactive protein (CRP) and interleukin 6 (IL-6) after access placement and at multiple times during 3 years' follow-up. Type of access was categorized as central venous catheter (CVC), arteriovenous graft (AVG), and arteriovenous fistula (AVF), and changes over time were recorded.
Predictor: Access type, age, sex, race, body mass index, diabetes, cardiovascular disease, and serum albumin level.
Outcomes: CRP level, IL-6 level, and mortality.
Measurements: We used mixed-effects pattern mixture models to study the association between access type and repeated measurements of inflammation and survival analysis to investigate the association of access type and mortality, adjusting for predictors.
Results: In a mixed-effects pattern mixture model, compared with AVFs, the presence of CVCs and AVGs was associated with 62% (P=0.02) and 30% (P=0.05) increases in average CRP levels, respectively. A Cox proportional hazards model yielded nonsignificant associations of CVC and AVG use (vs AVFs) with risk of mortality when adjusted for inflammatory marker levels. Higher CRP levels were associated with increased risk of CVC failure than lower CRP levels.
Limitations: CRP and IL-6 measurements not performed for all hemodialysis patients.
Conclusions: CVCs, compared with AVFs, are associated with a greater state of inflammation in incident hemodialysis patients, and the association of catheter use and mortality may be mediated by access-induced inflammation. Our findings support recommendations for the early removal or avoidance of CVC placements.
Keywords: C-reactive protein (CRP); Cox proportional hazard model; access failure; access patency; biomarker; central venous catheter (CVC); end-stage renal disease (ESRD); hemodialysis; inflammation; interleukin 6 (IL-6); mixed-effects model; vascular access type.
Copyright © 2014 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures


References
-
- National Kidney Foundation: NKF-DOQI clinical practice guidelines for vascular access. National Kidney Foundation-Dialysis Outcomes Quality Initiative. Am J Kidney Dis. 1997;30(4 Suppl 3):S150–S191. - PubMed
-
- Allon M, Robbin ML. Increasing arteriovenous fistulas in hemodialysis patients: problems and solutions. Kidney Int. 2002;62:1109–1124. - PubMed
-
- Churchill DN, Taylor DW, Cook RJ, et al. Canadian Hemodialysis Morbidity Study. Am J Kidney Dis. 1992;19:214–234. - PubMed
-
- Twardowski ZJ. Percutaneous blood access for hemodialysis. Semin Dial. 1995;8:175–186.
-
- Powe NR, Jaar B, Furth SL. Septicaemia in dialysis patients: Incidence, risk factors, and prognosis. Kidney Int. 1999;55:1081–1090. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
