

Clinical management of Staphylococcus aureus bacteremia: a review
- PMID: 25268440
- PMCID: PMC4263314
- DOI: 10.1001/jama.2014.9743
Clinical management of Staphylococcus aureus bacteremia: a review
Abstract
Importance: Several management strategies may improve outcomes in patients with Staphylococcus aureus bacteremia.
Objectives: To review evidence of management strategies for S. aureus bacteremia to determine whether transesophageal echocardiography is necessary in all adult cases and what is the optimal antibiotic therapy for methicillin-resistant S. aureus (MRSA) bacteremia.
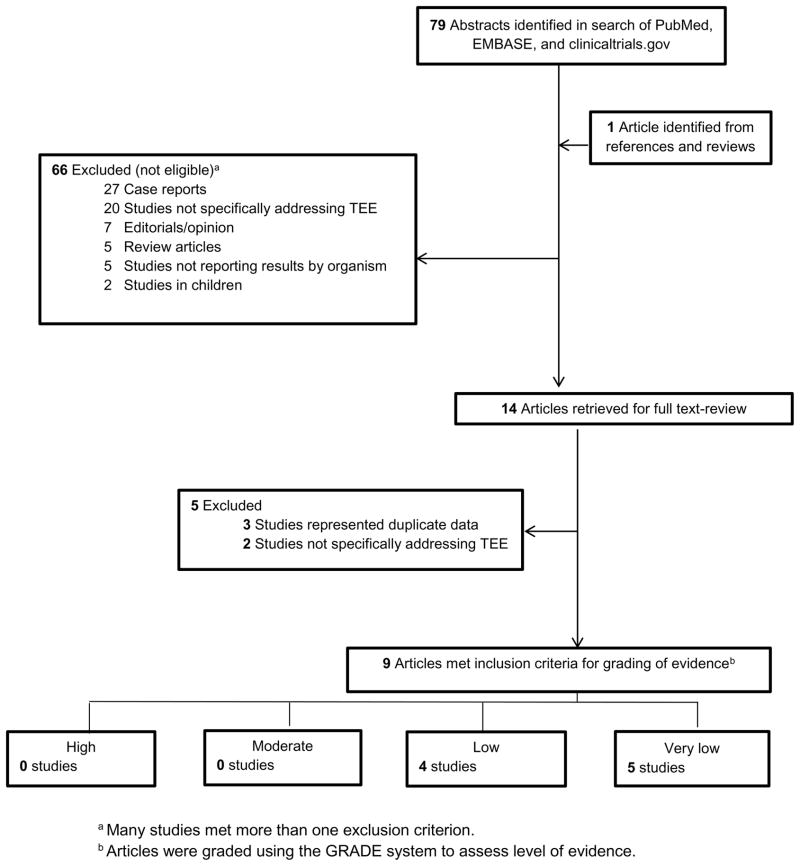
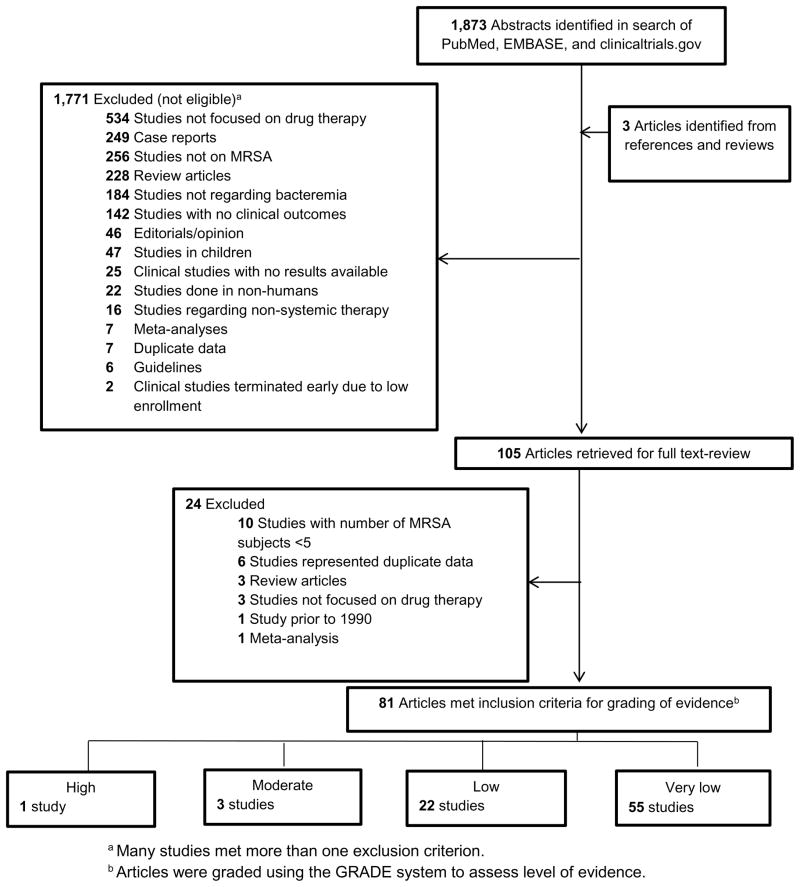
Evidence review: A PubMed search from inception through May 2014 was performed to identify studies addressing the role of transesophageal echocardiography in S. aureus bacteremia. A second search of PubMed, EMBASE, and the Cochrane Library from January 1990 through May 2014 was performed to find studies addressing antibiotic treatment for MRSA bacteremia. Studies reporting outcomes from antibiotic therapy for MRSA bacteremia were included. All searches, which were limited to English and focused on adults, were augmented by review of bibliographic references from included studies. The quality of evidence was assessed using the Grades of Recommendation, Assessment, Development and Evaluation system with consensus of independent evaluations by at least 2 of the authors.
Findings: In 9 studies with a total of 4050 patients, use of transesophageal echocardiography was associated with higher rates of a diagnosis of endocarditis (14%-28%) compared with transthoracic echocardiography (2%-15%). In 4 studies, clinical or transthoracic echocardiography findings did not predict subsequent transesophageal echocardiography findings of endocarditis. Five studies identified clinical or transthoracic echocardiography characteristics associated with low risk of endocarditis (negative predictive values from 93% to 100%). Characteristics associated with a low risk of endocarditis include absence of a permanent intracardiac device, sterile follow-up blood cultures within 4 days after the initial set, no hemodialysis dependence, nosocomial acquisition of S. aureus bacteremia, absence of secondary foci of infection, and no clinical signs of infective endocarditis. Of 81 studies of antibiotic therapy for MRSA bacteremia, only 1 high-quality trial was identified. In that study of 246 patients with S. aureus bacteremia, daptomycin was not inferior to vancomycin or an antistaphylococcal penicillin, each in combination with low-dose, short-course gentamicin (clinical success rate, 44.2% [53/120] vs 41.7% [48/115]; absolute difference, 2.4% [95% CI, -10.2% to 15.1%]).
Conclusions and relevance: All adult patients with S. aureus bacteremia should undergo echocardiography. Characteristics of low-risk patients with S. aureus bacteremia for whom transesophageal echocardiography can be safely avoided have been identified. Vancomycin and daptomycin are the first-line antibiotic choices for MRSA bacteremia. Well-designed studies to address the management of S. aureus bacteremia are needed.
Figures
Comment in
-
Diagnosing endocarditis in patients with Staphylococcus aureus bacteremia.JAMA. 2015 Jan 27;313(4):420. doi: 10.1001/jama.2014.16951. JAMA. 2015. PMID: 25626043 No abstract available.
-
Diagnosing endocarditis in patients with Staphylococcus aureus bacteremia--reply.JAMA. 2015 Jan 27;313(4):420-1. doi: 10.1001/jama.2014.16954. JAMA. 2015. PMID: 25626044 No abstract available.
-
Staphylococcus aureus bacteraemia management: where do we stand and where are we going?Evid Based Med. 2015 Aug;20(4):126. doi: 10.1136/ebmed-2014-110122. Epub 2015 Apr 20. Evid Based Med. 2015. PMID: 25895528 No abstract available.
References
-
- Cosgrove SE, Sakoulas G, Perencevich EN, Schwaber MJ, Karchmer AW, Carmeli Y. Comparison of mortality associated with methicillin-resistant and methicillin-susceptible Staphylococcus aureus bacteremia: a meta-analysis. Clin Infect Dis. 2003;36(1):53–59. - PubMed
-
- Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the infectious diseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis. 2011;52(3):e18–55. - PubMed
-
- Gould FK, Brindle R, Chadwick PR, et al. Guidelines (2008) for the prophylaxis and treatment of methicillin-resistant Staphylococcus aureus (MRSA) infections in the United Kingdom. J Antimicrob Chemother. 2009;63(5):849–861. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
