

Neutrophil/Lymphocyte ratio is associated with non-calcified plaque burden in patients with coronary artery disease
- PMID: 25268632
- PMCID: PMC4182451
- DOI: 10.1371/journal.pone.0108183
Neutrophil/Lymphocyte ratio is associated with non-calcified plaque burden in patients with coronary artery disease
Abstract
Background: Elevations in soluble markers of inflammation and changes in leukocyte subset distribution are frequently reported in patients with coronary artery disease (CAD). Lately, the neutrophil/lymphocyte ratio has emerged as a potential marker of both CAD severity and cardiovascular prognosis.
Objectives: The aim of the study was to investigate whether neutrophil/lymphocyte ratio and other immune-inflammatory markers were related to plaque burden, as assessed by coronary computed tomography angiography (CCTA), in patients with CAD.
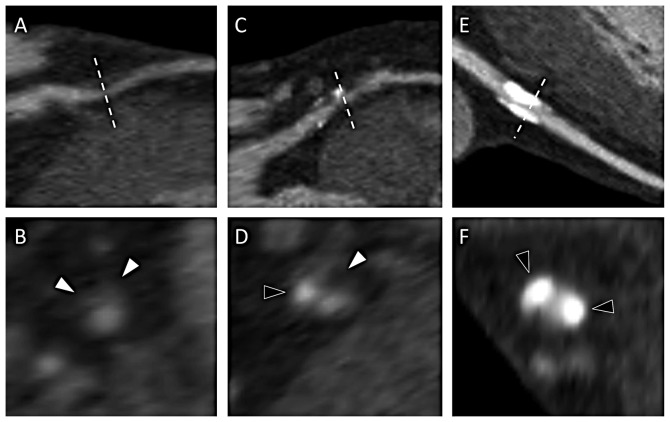
Methods: Twenty patients with non-ST-elevation acute coronary syndrome (NSTE-ACS) and 30 patients with stable angina (SA) underwent CCTA at two occasions, immediately prior to coronary angiography and after three months. Atherosclerotic plaques were classified as calcified, mixed and non-calcified. Blood samples were drawn at both occasions. Leukocyte subsets were analyzed by white blood cell differential counts and flow cytometry. Levels of C-reactive protein (CRP) and interleukin(IL)-6 were measured in plasma. Blood analyses were also performed in 37 healthy controls.
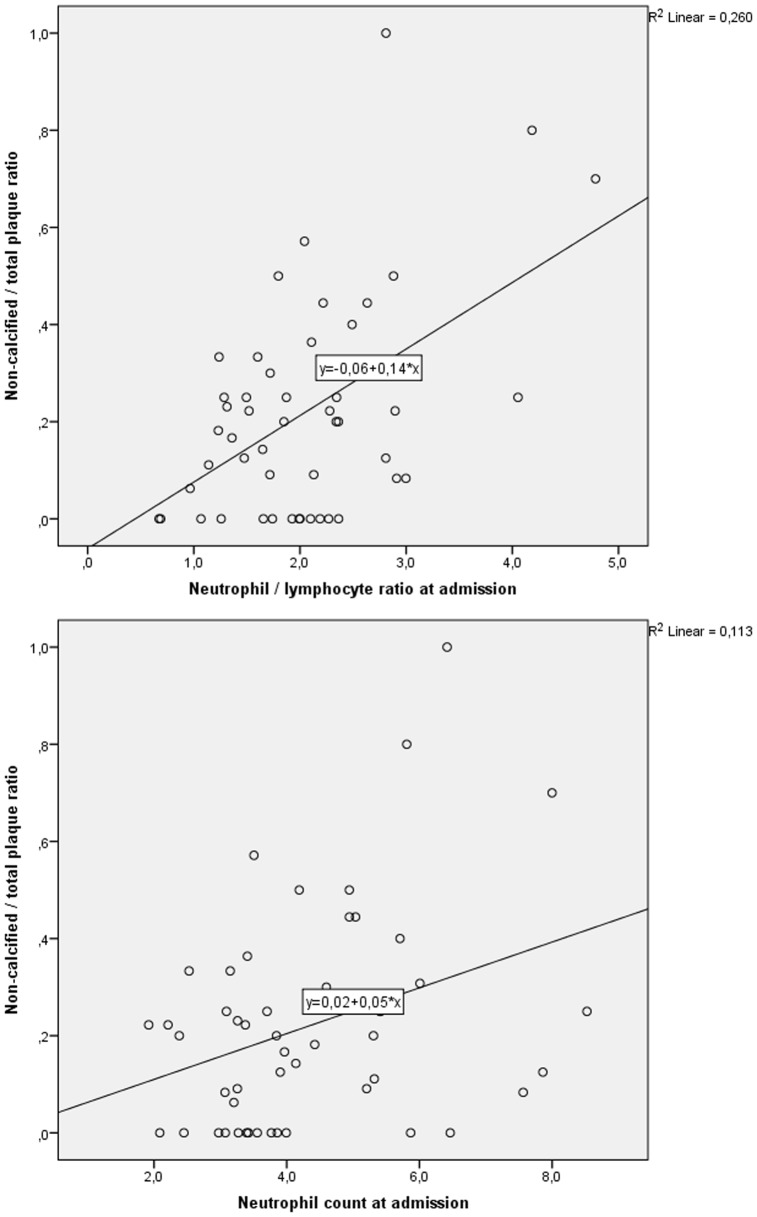
Results: Plaque variables did not change over 3 months, total plaque burden being similar in NSTE-ACS and SA. However, non-calcified/total plaque ratio was higher in NSTE-ACS, 0.25(0.09-0.44) vs 0.11(0.00-0.25), p<0.05. At admission, levels of monocytes, neutrophils, neutrophil/lymphocyte ratios, CD4+ T cells, CRP and IL-6 were significantly elevated, while levels of NK cells were reduced, in both patient groups as compared to controls. After 3 months, levels of monocytes, neutrophils, neutrophil/lymphocyte ratios and CD4+ T cells remained elevated in patients. Neutrophil/lymphocyte ratios and neutrophil counts correlated significantly with numbers of non-calcified plaques and also with non-calcified/total plaque ratio (r = 0.403, p = 0.010 and r = 0.382, p = 0.024, respectively), but not with total plaque burden.
Conclusions: Among immune-inflammatory markers in NSTE-ACS and SA patients, neutrophil counts and neutrophil/lymphocyte ratios were significantly correlated with non-calcified plaques. Data suggest that these easily measured biomarkers reflect the burden of vulnerable plaques in CAD.
Conflict of interest statement
Figures
References
-
- Hansson GK (2005) Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med 352: 1685–95. - PubMed
-
- Pai JK, Pischon T, Ma J, Manson JE, Hankinson SE, et al. (2004) Inflammatory markers and the risk of coronary heart disease in men and women. N Engl J Med 351: 2599–610. - PubMed
-
- Nijm J, Wikby A, Tompa A, Olsson AG, Jonasson L (2005) Circulating levels of proinflammatory cytokines and neutrophil-platelet aggregates in patients with coronary artery disease. Am J Cardiol 95(4): 452–6. - PubMed
-
- Jonasson L, Backteman K, Ernerudh J (2005) Loss of natural killer cell activity in patients with coronary artery disease. Atherosclerosis 183(2): 316–21. - PubMed
-
- Packard RR, Libby P (2008) Inflammation in atherosclerosis: from vascular biology to biomarker discovery and risk prediction. Clin Chem 54(1): 24–38. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
