

Cost-utility of cognitive behavioral therapy versus U.S. Food and Drug Administration recommended drugs and usual care in the treatment of patients with fibromyalgia: an economic evaluation alongside a 6-month randomized controlled trial
- PMID: 25270426
- PMCID: PMC4203881
- DOI: 10.1186/s13075-014-0451-y
Cost-utility of cognitive behavioral therapy versus U.S. Food and Drug Administration recommended drugs and usual care in the treatment of patients with fibromyalgia: an economic evaluation alongside a 6-month randomized controlled trial
Abstract
Introduction: Cognitive behavioral therapy (CBT) and U.S. Food and Drug Administration (FDA)-recommended pharmacologic treatments (RPTs; pregabalin, duloxetine, and milnacipran) are effective treatment options for fibromyalgia (FM) syndrome and are currently recommended by clinical guidelines. We compared the cost-utility from the healthcare and societal perspectives of CBT versus RPT (combination of pregabalin + duloxetine) and usual care (TAU) groups in the treatment of FM.
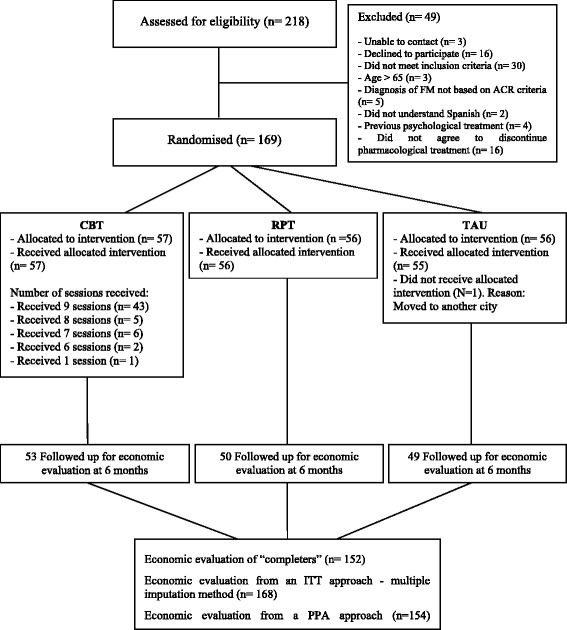
Methods: The economic evaluation was conducted alongside a 6-month, multicenter, randomized, blinded, parallel group, controlled trial. In total, 168 FM patients from 41 general practices in Zaragoza (Spain) were randomized to CBT (n = 57), RPT (n = 56), or TAU (n = 55). The main outcome measures were Quality-Adjusted Life Years (QALYs, assessed by using the EuroQoL-5D questionnaire) and improvements in health-related quality of life (HRQoL, assessed by using EuroQoL-5D visual analogue scale, EQ-VAS). The costs of healthcare use were estimated from patient self-reports (Client Service Receipt Inventory). Cost-utility was assessed by using the net-benefit approach and cost-effectiveness acceptability curves (CEACs).
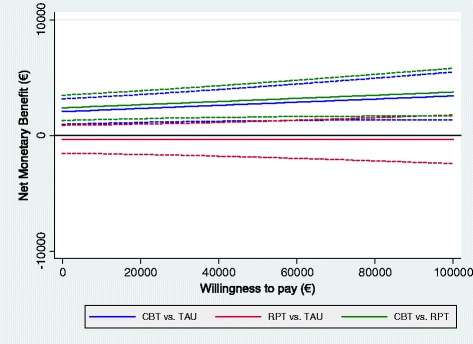
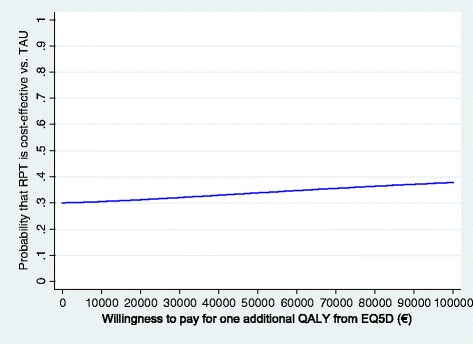
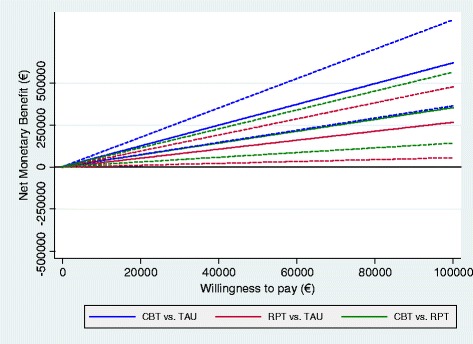
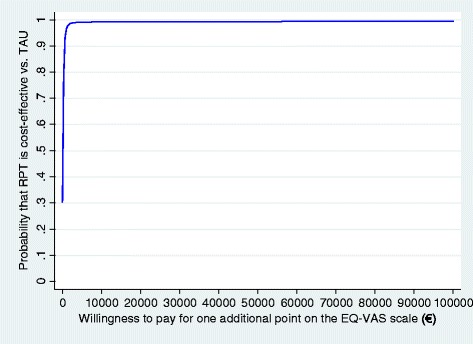
Results: On average, the total costs per patient in the CBT group (1,847 €) were significantly lower than those in patients receiving RPT (3,664 €) or TAU (3,124 €). Patients receiving CBT reported a higher quality of life (QALYs and EQ-VAS scores); the differences between groups were significant only for EQ-VAS. From a complete case-analysis approach (base case), the point estimates of the cost-effectiveness ratios resulted in dominance for the CBT group in all of the comparisons performed, by using both QALYs and EQ-VAS as outcomes. These findings were confirmed by bootstrap analyses, net-benefit curves, and CEACs. Two additional sensitivity analyses (intention-to-treat analysis and per-protocol analysis) indicated that the results were robust. The comparison of RPT with TAU yielded no clear preference for either treatment when using QALYs, although RPT was determined to be more cost-effective than TAU when evaluating EQ-VAS.
Conclusions: Because of lower costs, CBT is the most cost-effective treatment for adult FM patients. Implementation in routine medical care would require policymakers to develop more-widespread public access to trained and experienced therapists in group-based forms of CBT.
Trial registration: Current Controlled Trials ISRCTN10804772. Registered 29 September 2008.
Figures
References
-
- Smith HS, Harris R, Clauw D. Fibromyalgia: an afferent processing disorder leading to a complex pain generalized syndrome. Pain Physician. 2011;14:E217–E245. - PubMed
-
- Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, Tugwell P, Campbell SM, Abeles M, Clar P. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia: report of the Multicenter Criteria Committee. Arthritis Rheum. 1990;33:160–172. doi: 10.1002/art.1780330203. - DOI - PubMed
-
- Wolfe F, Clauw DJ, Fitzcharles M-A, Goldenberg DL, Katz RS, Mease P, Russell AS, Russell IJ, Winfield JB, Yunus MB. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res (Hoboken) 2010;62:600–610. doi: 10.1002/acr.20140. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
