

Treatment of autoimmune hemolytic anemias
- PMID: 25271314
- PMCID: PMC4181250
- DOI: 10.3324/haematol.2014.114561
Treatment of autoimmune hemolytic anemias
Abstract
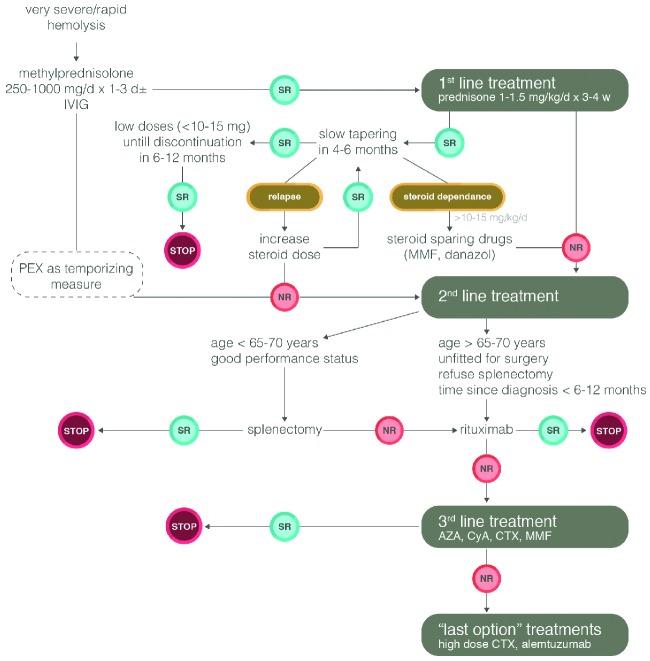
Autoimmune hemolytic anemia (AIHA) is a relatively uncommon disorder caused by autoantibodies directed against self red blood cells. It can be idiopathic or secondary, and classified as warm, cold (cold hemagglutinin disease (CAD) and paroxysmal cold hemoglobinuria) or mixed, according to the thermal range of the autoantibody. AIHA may develop gradually, or have a fulminant onset with life-threatening anemia. The treatment of AIHA is still not evidence-based. The first-line therapy for warm AIHA are corticosteroids, which are effective in 70-85% of patients and should be slowly tapered over a time period of 6-12 months. For refractory/relapsed cases, the current sequence of second-line therapy is splenectomy (effective approx. in 2 out of 3 cases but with a presumed cure rate of up to 20%), rituximab (effective in approx. 80-90% of cases), and thereafter any of the immunosuppressive drugs (azathioprine, cyclophosphamide, cyclosporin, mycophenolate mofetil). Additional therapies are intravenous immunoglobulins, danazol, plasma-exchange, and alemtuzumab and high-dose cyclophosphamide as last resort option. As the experience with rituximab evolves, it is likely that this drug will be located at an earlier point in therapy of warm AIHA, before more toxic immunosuppressants, and in place of splenectomy in some cases. In CAD, rituximab is now recommended as first-line treatment.
Copyright© Ferrata Storti Foundation.
Figures
References
-
- Petz LD, Garratty G. Immune Hemolytic Anemias. 2nd ed Philadelphia: Churchill Livingstone; 2004
-
- Lechner K, Jager U. How I treat autoimmune hemolytic anemias in adults. Blood. 2010;16:1831–8 - PubMed
-
- Valent P, Lechner K. Diagnosis and treatment of autoimmune haemolytic anaemias in adults: a clinical review. Wien Klin Wochenschr. 2008;120:136–51 - PubMed
-
- Silberstein LE, Cunningham MJ. Autoimmune Hemolytic Anemias. In: Hillyer CD, Silberstein LE, Ness PM, Anderson KC, Roback JD. (eds). Blood Banking and Transfusion Medicine. Basic Principles and Practice. 2nd ed Philadelphia: Churchill Livingstone; 2007
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
