

doi: 10.1164/rccm.201405-0993LE.
Phrenic nerve stimulation increases human diaphragm fiber force after cardiothoracic surgery
Affiliations
- PMID: 25271750
- PMCID: PMC4299610
- DOI: 10.1164/rccm.201405-0993LE
Item in Clipboard
Phrenic nerve stimulation increases human diaphragm fiber force after cardiothoracic surgery
Am J Respir Crit Care Med.
.
No abstract available
Figures
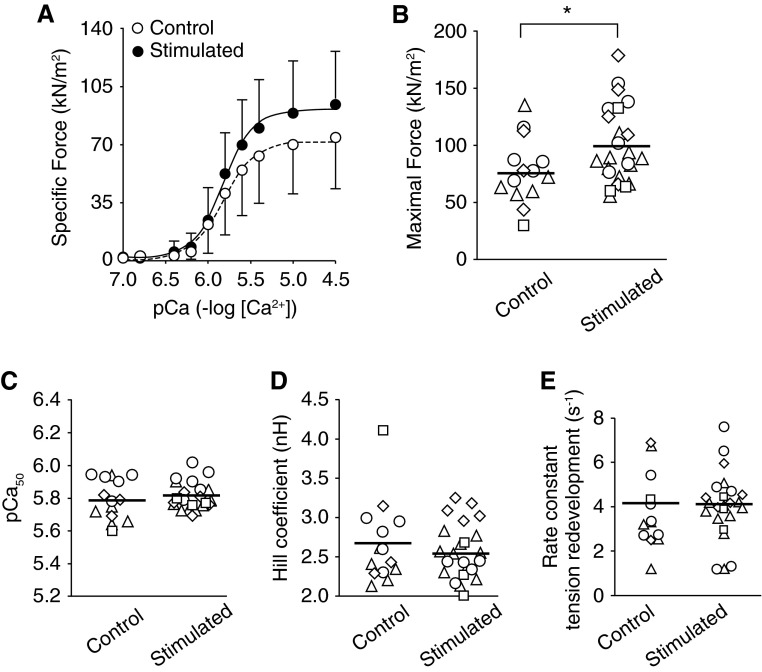
Phrenic nerve stimulation increases diaphragm fiber force after cardiothoracic surgery. (A) Specific force versus pCa relationship for all fibers from control and stimulated hemidiaphragms. Specific force is absolute force (in kilonewtons) normalized to the fiber cross-sectional area (in meters squared). pCa is the negative log[Ca2+], and in the figure shown, [Ca2+] ranges from 0.1 to 32 μM. Symbols and error bars are mean ± standard deviation. Solid and dashed lines are best fit from Hill equation. (B) Maximal calcium-activated (pCa 4.5) specific force. (C) pCa50 is pCa that elicits 50% maximal force and represents calcium sensitivity of the contractile apparatus. (D) Hill coefficient is equivalent to the slope of force–pCa relationship and represents the cooperativity of thin-filament activation. (E) Rate constant of tension redevelopment (ktr) obtained from quick-release and restretch test. The ktr is an indicator of cross-bridge cycling kinetics. (B–E) Data are for each individual fiber studied (symbols) and mean for condition (solid line). The four unique symbols shown represent fibers from each patient. *P < 0.05 determined by linear mixed model as detailed in the text.
References
-
- Jaber S, Petrof BJ, Jung B, Chanques G, Berthet JP, Rabuel C, Bouyabrine H, Courouble P, Koechlin-Ramonatxo C, Sebbane M, et al. Rapidly progressive diaphragmatic weakness and injury during mechanical ventilation in humans. Am J Respir Crit Care Med. 2011;183:364–371. - PubMed
-
- Welvaart WN, Paul MA, Stienen GJ, van Hees HW, Loer SA, Bouwman R, Niessen H, de Man FS, Witt CC, Granzier H, et al. Selective diaphragm muscle weakness after contractile inactivity during thoracic surgery. Ann Surg. 2011;254:1044–1049. - PubMed
-
- Powers SK, Wiggs MP, Sollanek KJ, Smuder AJ. Ventilator-induced diaphragm dysfunction: cause and effect. Am J Physiol Regul Integr Comp Physiol. 2013;305:R464–R477. - PubMed
-
- Masmoudi H, Coirault C, Demoule A, Mayaux J, Beuvin M, Romero N, Assouad J, Similowski T. Can phrenic stimulation protect the diaphragm from mechanical ventilation-induced damage? Eur Respir J. 2013;42:280–283. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
