

New strategies in acute promyelocytic leukemia: moving to an entirely oral, chemotherapy-free upfront management approach
- PMID: 25274377
- PMCID: PMC4882758
- DOI: 10.1158/1078-0432.CCR-13-2725
New strategies in acute promyelocytic leukemia: moving to an entirely oral, chemotherapy-free upfront management approach
Abstract
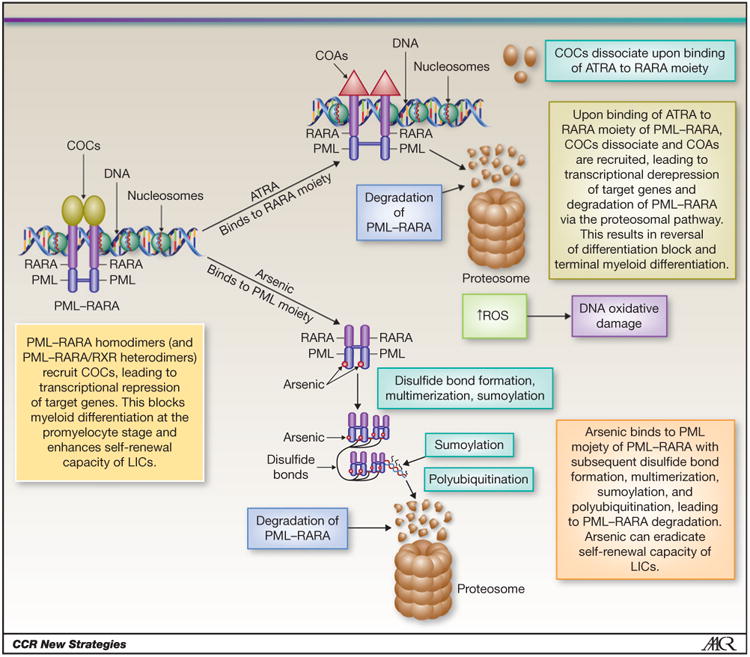
Incorporation of all-trans retinoic acid (ATRA) and arsenic trioxide (ATO) into the management paradigms of acute promyelocytic leukemia (APL) has markedly improved outcomes. Significant progress occurred in understanding the molecular pathogenesis of APL. ATO, in contrast with ATRA, is capable of eradicating the APL-initiating cells and can result in cure. Preclinical and clinical data confirmed the synergy of ATO and ATRA, and the ATRA-ATO combination was proved noninferior to a standard ATRA-chemotherapy regimen in patients with non-high-risk APL. Oral formulations of arsenic exhibited excellent activity in advanced clinical testing and their combinations with ATRA offer an opportunity for a completely oral, chemotherapy-free regimen for curing APL. Nonetheless, significant challenges remain. Reducing early death due to bleeding complications is an important area of unmet need. Data suggest that delays in initiation of ATRA upon suspecting APL continue to occur in the community and contribute to early mortality. Questions remain about the optimal place and schedule of arsenic in the therapeutic sequence and the role of the oral formulations. Refining the role of minimal residual disease in directing treatment decisions is important. Development of novel targeted agents to treat relapsed disease requires deeper understanding of the secondary resistance mechanisms to ATRA and ATO.
©2014 American Association for Cancer Research.
Conflict of interest statement
Figures
Similar articles
-
Contemporary treatment of APL.Curr Hematol Malig Rep. 2014 Jun;9(2):193-201. doi: 10.1007/s11899-014-0205-6. Curr Hematol Malig Rep. 2014. PMID: 24643310 Free PMC article. Review.
-
Role of arsenic trioxide in acute promyelocytic leukemia.Curr Treat Options Oncol. 2013 Jun;14(2):170-84. doi: 10.1007/s11864-012-0223-3. Curr Treat Options Oncol. 2013. PMID: 23322117
-
Chemotherapy-free approaches to newly-diagnosed acute promyelocytic leukaemia: is oral-arsenic trioxide/all-trans retinoic acid/ascorbic acid the answer?Expert Rev Hematol. 2024 Oct;17(10):661-667. doi: 10.1080/17474086.2024.2391098. Epub 2024 Aug 12. Expert Rev Hematol. 2024. PMID: 39120131 Review.
-
An efficient therapeutic approach to patients with acute promyelocytic leukemia using a combination of arsenic trioxide with low-dose all-trans retinoic acid.Hematol Oncol. 2004 Jun;22(2):63-71. doi: 10.1002/hon.728. Hematol Oncol. 2004. PMID: 15468344 Review.
-
Prolonged treatment with arsenic trioxide (ATO) and all-trans-retinoic acid (ATRA) for relapsed acute promyelocytic leukemia previously treated with ATRA and chemotherapy.Ann Hematol. 2018 Oct;97(10):1797-1802. doi: 10.1007/s00277-018-3400-z. Epub 2018 Jun 27. Ann Hematol. 2018. PMID: 29951912
Cited by
-
Acute promyelocytic leukemia: where did we start, where are we now, and the future.Blood Cancer J. 2015 Apr 17;5(4):e304. doi: 10.1038/bcj.2015.25. Blood Cancer J. 2015. PMID: 25885425 Free PMC article. Review.
-
Natural variation in C. elegans arsenic toxicity is explained by differences in branched chain amino acid metabolism.Elife. 2019 Apr 8;8:e40260. doi: 10.7554/eLife.40260. Elife. 2019. PMID: 30958264 Free PMC article.
-
Real-life experience of a brief arsenic trioxide-based consolidation chemotherapy in the management of acute promyelocytic leukemia: favorable outcomes with limited anthracycline exposure and shorter consolidation therapy.Clin Lymphoma Myeloma Leuk. 2015 May;15(5):292-7. doi: 10.1016/j.clml.2014.11.001. Epub 2014 Nov 15. Clin Lymphoma Myeloma Leuk. 2015. PMID: 25499624 Free PMC article.
-
Retinoic acid and arsenic trioxide induce lasting differentiation and demethylation of target genes in APL cells.Sci Rep. 2019 Jul 1;9(1):9414. doi: 10.1038/s41598-019-45982-7. Sci Rep. 2019. PMID: 31263158 Free PMC article.
-
Therapeutic Approaches for Acute Promyelocytic Leukaemia: Moving Towards an Orally Chemotherapy-Free Era.Front Oncol. 2020 Oct 20;10:586004. doi: 10.3389/fonc.2020.586004. eCollection 2020. Front Oncol. 2020. PMID: 33194735 Free PMC article. Review.
References
-
- Wang ZY, Chen Z. Acute promyelocytic leukemia: from highly fatal to highly curable. Blood. 2008;111:2505–15. - PubMed
-
- de The H, Chomienne C, Lanotte M, Degos L, Dejean A. The t(15;17) translocation of acute promyelocytic leukaemia fuses the retinoic acid receptor alpha gene to a novel transcribed locus. Nature. 1990;347:558–61. - PubMed
-
- Tomita A, Kiyoi H, Naoe T. Mechanisms of action and resistance to all-trans retinoic acid (ATRA) and arsenic trioxide (As2O3) in acute promyelocytic leukemia. Int J Hematol. 2013;97:717–25. - PubMed
-
- Licht JD, Chomienne C, Goy A, Chen A, Scott AA, Head DR, et al. Clinical and molecular characterization of a rare syndrome of acute promyelocytic leukemia associated with translocation (11;17) Blood. 1995;85:1083–94. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
