Macular hole formation in rhegmatogenous retinal detachment after scleral buckling
- PMID: 25276077
- PMCID: PMC4179112
- DOI: 10.3341/kjo.2014.28.5.364
Macular hole formation in rhegmatogenous retinal detachment after scleral buckling
Abstract
Purpose: To describe early macular hole (MH) development in rhegmatogenous retinal detachment (RRD) after scleral buckling (SB) based on optical coherence tomography (OCT) findings.
Methods: The medical records and spectral domain OCT images of patients in whom MH developed after RRD repair were evaluated retrospectively.
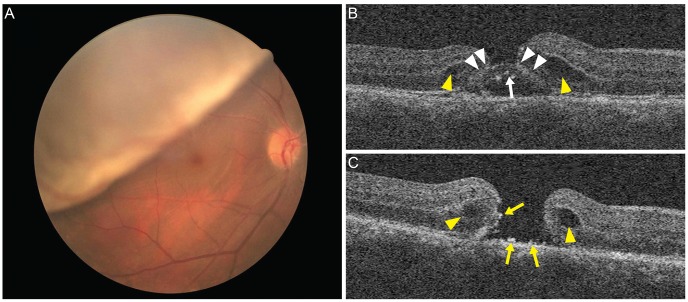
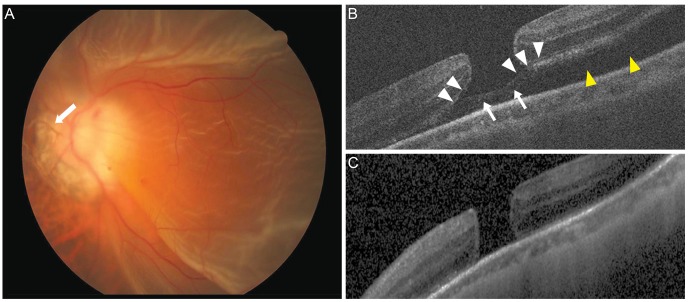
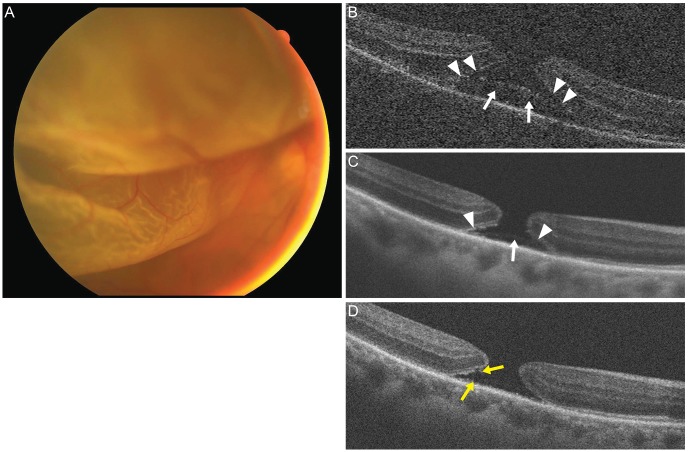
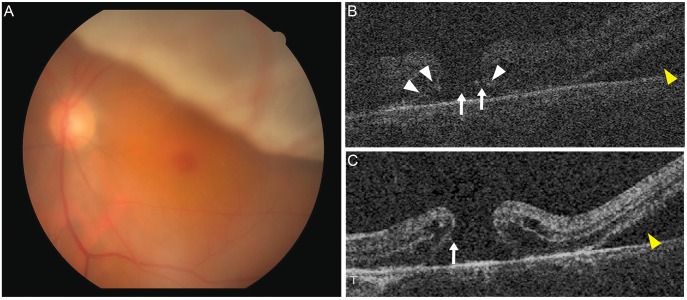
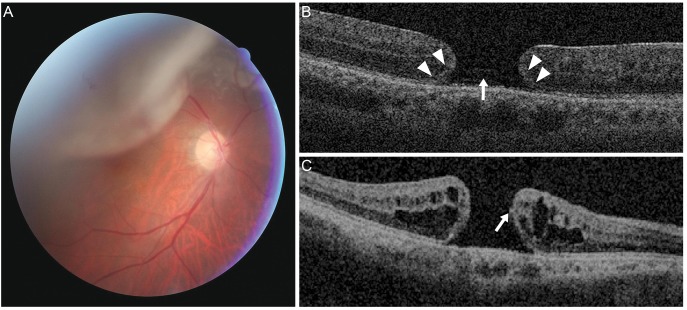
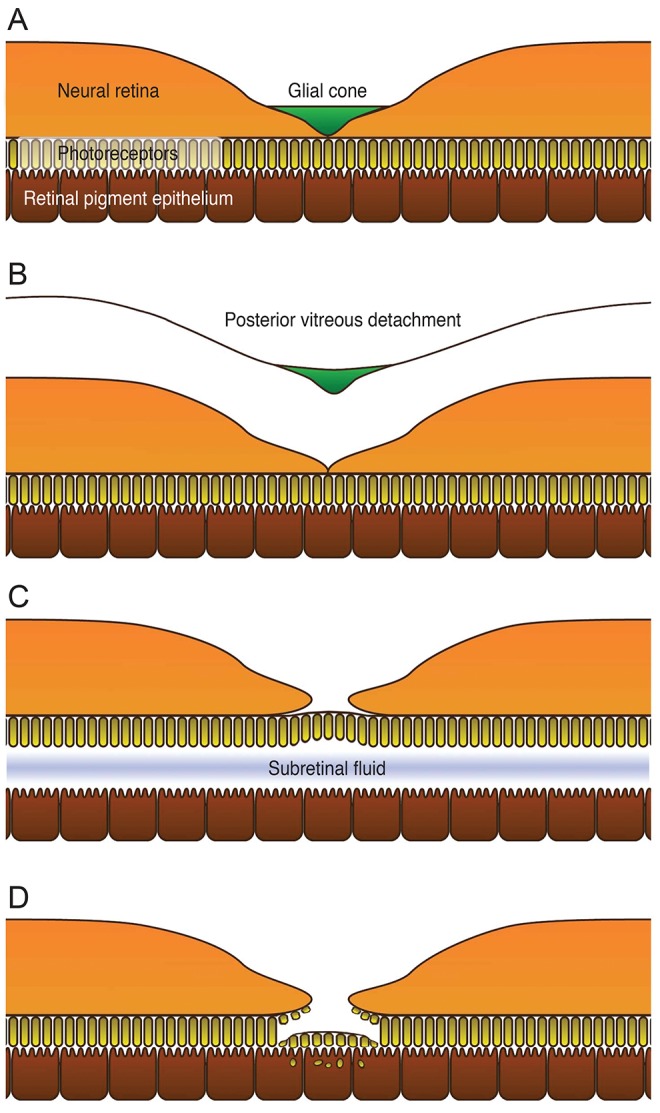
Results: A postoperative MH was detected in five eyes that underwent SB during a 6-year period. All had fovea-off RRD without MH at the time of surgery. OCT showed partial loss of the inner retina with a preserved photoreceptor layer in early postoperative days. On average, 7 days (range,5 to 8 days) after surgery, outer retinal tissues disappeared, resulting in the full-thickness MH.
Conclusions: Serial OCT findings revealed that partial-thickness lamellar holes progressed to full-thickness MHs, which were formed by the degeneration of the outer retina in eyes with preceding loss of the glial cone in the fovea.
Keywords: Retinal perforations; Rhegmatogenous retinal detachment; Scleral buckling.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Gass JD. Reappraisal of biomicroscopic classification of stages of development of a macular hole. Am J Ophthalmol. 1995;119:752–759. - PubMed
-
- Gaudric A, Haouchine B, Massin P, et al. Macular hole formation: new data provided by optical coherence tomography. Arch Ophthalmol. 1999;117:744–751. - PubMed
-
- Smiddy WE, Flynn HW., Jr Pathogenesis of macular holes and therapeutic implications. Am J Ophthalmol. 2004;137:525–537. - PubMed
-
- Johnson MW. Posterior vitreous detachment: evolution and complications of its early stages. Am J Ophthalmol. 2010;149:371–382. - PubMed
-
- Haouchine B, Massin P, Gaudric A. Foveal pseudocyst as the first step in macular hole formation: a prospective study by optical coherence tomography. Ophthalmology. 2001;108:15–22. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical