

Introducing an integrated intermediate care unit improves ICU utilization: a prospective intervention study
- PMID: 25276092
- PMCID: PMC4177684
- DOI: 10.1186/1471-2253-14-76
Introducing an integrated intermediate care unit improves ICU utilization: a prospective intervention study
Abstract
Background: Improvement of appropriate bed use and access to intensive care (ICU) beds is essential in optimizing utilization of ICU capacity. The introduction of an intermediate care unit (IMC) integrated in the ICU care may improve this utilization.
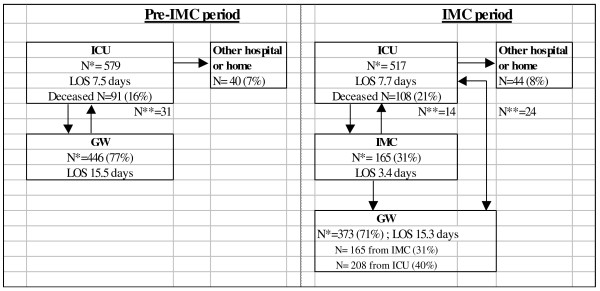
Method: In a before-after prospective intervention study in a university hospital mixed ICU, the impact of introducing a six-bed mixed IMC unit supervised and staffed by ICU physicians was investigated. Changes in ICU utilization (length of stay, frequency of mechanical ventilation use), nursing workload assessed byTISS-28 score, as well as inappropriate bed use, accessibility of the ICU (number of referrals), and clinical outcome indicators (readmission and mortality rates) were measured.
Results: During 17 months, data of 1027 ICU patients were collected. ICU utilization improved significantly with an increased appropriate use of ICU beds. However, the number of referrals, readmissions to the ICU and mortality rates did not decrease after the IMC was opened.
Conclusion: The IMC contributed to a more appropriate use of ICU facilities and did result in a significant increase in mean nursing workload at the ICU.
Keywords: Efficiency; Hospital bed capacity; Intensive care; Intermediate care; Resource allocation.
Figures
References
-
- Bone RC, McElwee NE, Eubanks DH, Gluck EH. Analysis of indications for early discharge from the intensive care unit. Clinical efficacy assessment project: American College of Physicians. Chest. 1993;104(6):8112–8117. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
