

Magnetic resonance imaging for lung cancer screen
- PMID: 25276380
- PMCID: PMC4178109
- DOI: 10.3978/j.issn.2072-1439.2014.08.43
Magnetic resonance imaging for lung cancer screen
Abstract
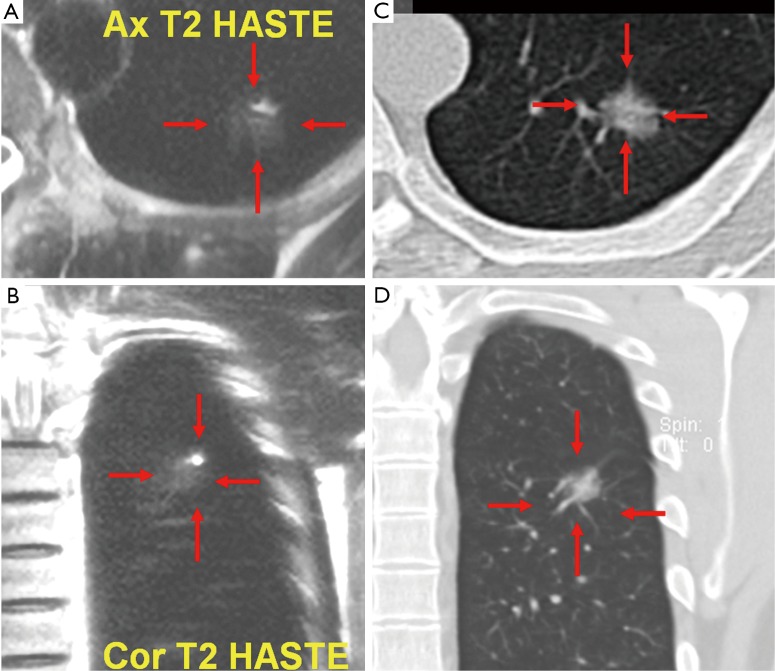
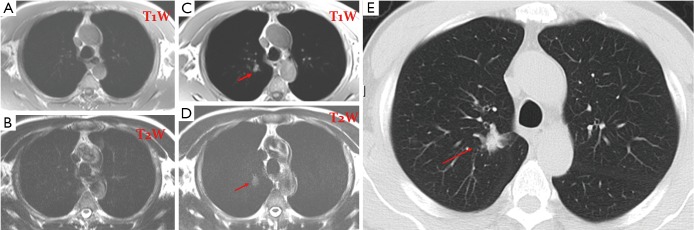
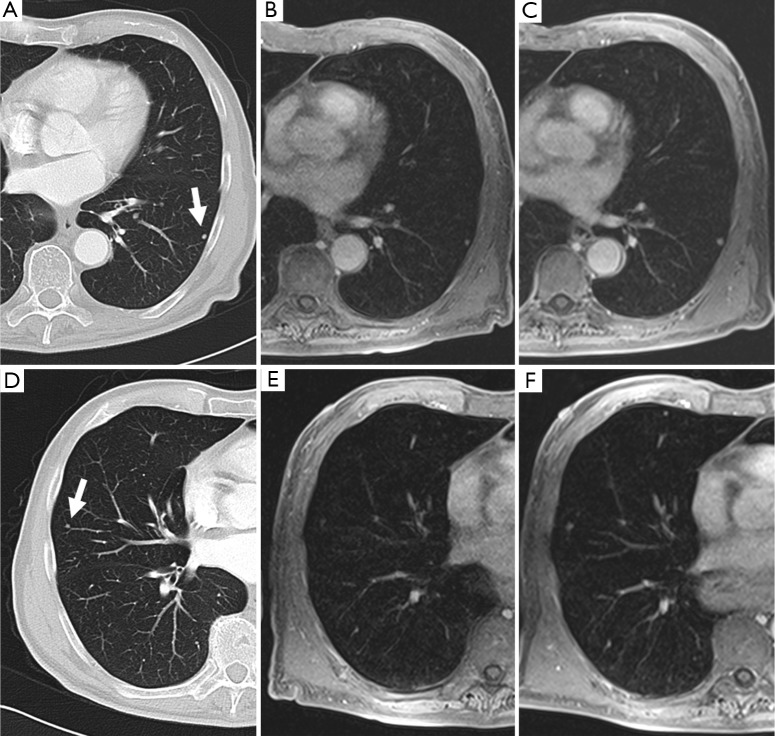
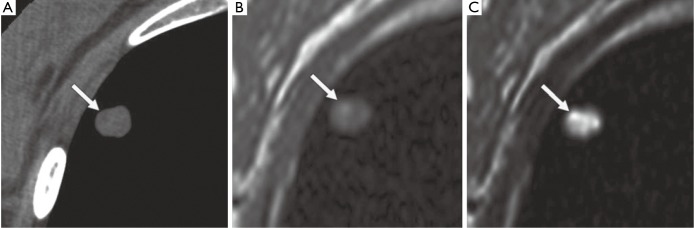
Lung cancer is the leading cause of cancer related death throughout the world. Lung cancer is an example of a disease for which a large percentage of the high-risk population can be easily identified via a smoking history. This has led to the investigation of lung cancer screening with low-dose helical/multi-detector CT. Evidences suggest that early detection of lung cancer allow more timely therapeutic intervention and thus a more favorable prognosis for the patient. The positive relationship of lesion size to likelihood of malignancy has been demonstrated previously, at least 99% of all nodules 4 mm or smaller are benign, while noncalcified nodules larger than 8 mm diameter bear a substantial risk of malignancy. In the recent years, the availability of high-performance gradient systems, in conjunction with phased-array receiver coils and optimized imaging sequences, has made MR imaging of the lung feasible. It can now be assumed a threshold size of 3-4 mm for detection of lung nodules with MRI under the optimal conditions of successful breath-holds with reliable gating or triggering. In these conditions, 90% of all 3-mm nodules can be correctly diagnosed and that nodules 5 mm and larger are detected with 100% sensitivity. Parallel imaging can significantly shorten the imaging acquisition time by utilizing the diversity of sensitivity profile of individual coil elements in multi-channel radiofrequency receive coil arrays or transmit/receive coil arrays to reduce the number of phase encoding steps required in imaging procedure. Compressed sensing technique accelerates imaging acquisition from dramatically undersampled data set by exploiting the sparsity of the images in an appropriate transform domain. With the combined imaging algorithm of parallel imaging and compressed sensing and advanced 32-channel or 64-channel RF hardware, overall imaging acceleration of 20 folds or higher can then be expected, ultimately achieve free-breathing and no ECG gating acquisitions in lung cancer MRI screening. Further development of protocols, more clinical trials and the use of advanced analysis tools will further evaluate the real significance of lung MRI.
Keywords: CT; Lung; MR; cancer; screening.
Figures
References
-
- Ferlay J, Shin HR, Bray F, et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 2010;127:2893-917 - PubMed
-
- Sone S, Takashima S, Li F, et al. Mass screening for lung cancer with mobile spiral computed tomography scanner. Lancet 1998;351:1242-5 - PubMed
-
- Heelan RT, Flehinger BJ, Melamed MR, et al. Non-small-cell lung cancer: results of the New York screening program. Radiology 1984;151:289-93 - PubMed
-
- Swensen SJ, Silverstein MD, Ilstrup DM, et al. The probability of malignancy in solitary pulmonary nodules. Application to small radiologically indeterminate nodules. Arch Intern Med 1997;157:849-55 - PubMed