

Are national policies and programs for prevention and management of postpartum hemorrhage and preeclampsia adequate? A key informant survey in 37 countries
- PMID: 25276587
- PMCID: PMC4168639
- DOI: 10.9745/GHSP-D-14-00034
Are national policies and programs for prevention and management of postpartum hemorrhage and preeclampsia adequate? A key informant survey in 37 countries
Abstract
Introduction: Although maternal mortality has declined substantially in recent years, efforts to address postpartum hemorrhage (PPH) and preeclampsia/eclampsia (PE/E) must be systematically scaled up in order for further reduction to take place. In 2012, a key informant survey was conducted to identify both national and global gaps in PPH and PE/E program priorities and to highlight focus areas for future national and global programming.
Methods: Between January and March 2012, national program teams in 37 countries completed a 44-item survey, consisting mostly of dichotomous yes/no responses and addressing 6 core programmatic areas: policy, training, medication distribution and logistics, national reporting of key indicators, programming, and challenges to and opportunities for scale up. An in-country focal person led the process to gather the necessary information from key local stakeholders. Some countries also provided national essential medicines lists and service delivery guidelines for comparison and further analysis.
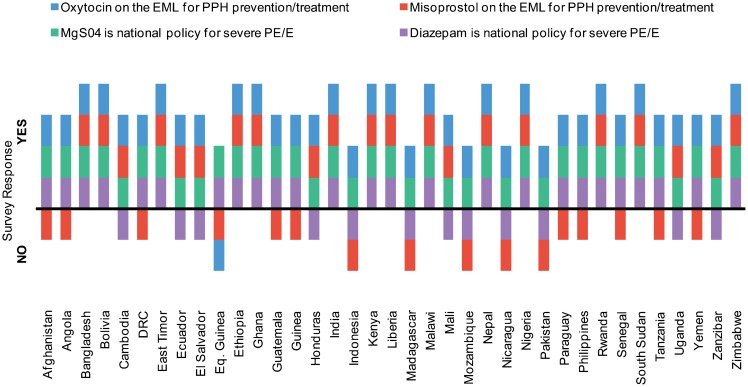
Results: Most surveyed countries have many elements in place to address PPH and PE/E, but notable gaps remain in both policy and practice. Oxytocin and magnesium sulfate were reported to be regularly available in facilities in 89% and 76% of countries, respectively. Only 27% of countries, however, noted regular availability of misoprostol in health facilities. Midwife scope of practice regarding PPH and PE/E is inconsistent with global norms in a number of countries: 22% of countries do not allow midwives to administer magnesium sulfate and 30% do not allow them to perform manual removal of the placenta.
Conclusions: Most countries surveyed have many of the essential policies and program elements to prevent/manage PPH and PE/E, but absence of commodities (especially misoprostol), limitations in scope of practice for midwives, and gaps in inclusion of maternal health indicators in the national data systems have impeded efforts to scale up programs nationally.
Figures






References
-
- World Health Organization (WHO); United Nations Children's Fund (UNICEF); United Nations Population Fund (UNFPA); World Bank. Trends in maternal mortality: 1990 to 2010: WHO, UNICEF, UNFPA and The World Bank estimates. Geneva: WHO; 2012. Available from: http://whqlibdoc.who.int/publications/2012/9789241503631_eng.pdf
-
- Every Woman Every Child [Internet]. New York: UN Commission on Life-Saving Commodities for Women and Children (UNCoLSC). Life-saving commodities; [cited 2014 Jan 7]. Available from: http://www.everywomaneverychild.org/resources/un-commission-on-life-savi...
-
- World Health Organization (WHO), Department of Reproductive Health and Research. WHO recommendations for the prevention and treatment of postpartum haemorrhage. Geneva: WHO; 2012. Available from: http://www.who.int/reproductivehealth/publications/maternal_perinatal_he... - PubMed
-
- World Health Organization (WHO). WHO recommendations for prevention and treatment of pre-eclampsia and eclampsia. Geneva: WHO; 2011. Available from: http://whqlibdoc.who.int/publications/2011/9789241548335_eng.pdf - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources