

Early versus delayed administration of norepinephrine in patients with septic shock
- PMID: 25277635
- PMCID: PMC4194405
- DOI: 10.1186/s13054-014-0532-y
Early versus delayed administration of norepinephrine in patients with septic shock
Abstract
Introduction: This study investigated the incidence of delayed norepinephrine administration following the onset of septic shock and its effect on hospital mortality.
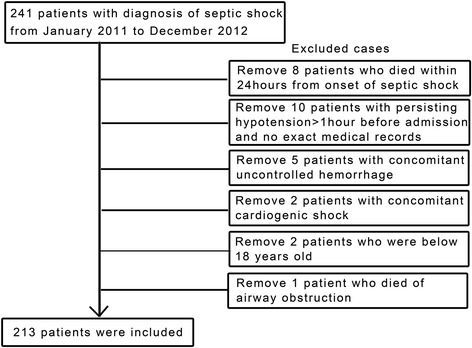
Methods: We conducted a retrospective cohort study using data from 213 adult septic shock patients treated at two general surgical intensive care units of a tertiary care hospital over a two year period. The primary outcome was 28-day mortality.
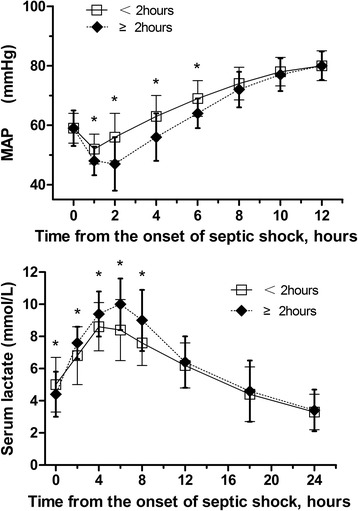
Results: The 28-day mortality was 37.6% overall. Among the 213 patients, a strong relationship between delayed initial norepinephrine administration and 28-day mortality was noted. The average time to initial norepinephrine administration was 3.1 ± 2.5 hours. Every 1-hour delay in norepinephrine initiation during the first 6 hours after septic shock onset was associated with a 5.3% increase in mortality. Twenty-eight day mortality rates were significantly higher when norepinephrine administration was started more than or equal to 2 hours after septic shock onset (Late-NE) compared to less than 2 hours (Early-NE). Mean arterial pressures at 1, 2, 4, and 6 hours after septic shock onset were significantly higher and serum lactate levels at 2, 4, 6, and 8 hours were significantly lower in the Early-NE than the Late-NE group. The duration of hypotension and norepinephrine administration was significantly shorter and the quantity of norepinephrine administered in a 24-hour period was significantly less for the Early-NE group compared to the Late-NE group. The time to initial antimicrobial treatment was not significantly different between the Early-NE and Late-NE groups.
Conclusion: Our results show that early administration of norepinephrine in septic shock patients is associated with an increased survival rate.
Figures



Comment in
-
Timing of norepinephrine in septic patients: NOT too little too late.Crit Care. 2014 Dec 15;18(6):691. doi: 10.1186/s13054-014-0691-x. Crit Care. 2014. PMID: 25672524 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
