

High-sensitivity troponin T and N-terminal pro-B-type natriuretic peptide (NT-proBNP) and risk of incident heart failure in patients with CKD: the Chronic Renal Insufficiency Cohort (CRIC) Study
- PMID: 25278510
- PMCID: PMC4378105
- DOI: 10.1681/ASN.2014010108
High-sensitivity troponin T and N-terminal pro-B-type natriuretic peptide (NT-proBNP) and risk of incident heart failure in patients with CKD: the Chronic Renal Insufficiency Cohort (CRIC) Study
Erratum in
-
Erratum.J Am Soc Nephrol. 2015 Oct;26(10):2599. doi: 10.1681/ASN.2015050575. J Am Soc Nephrol. 2015. PMID: 26424867 Free PMC article. No abstract available.
Abstract
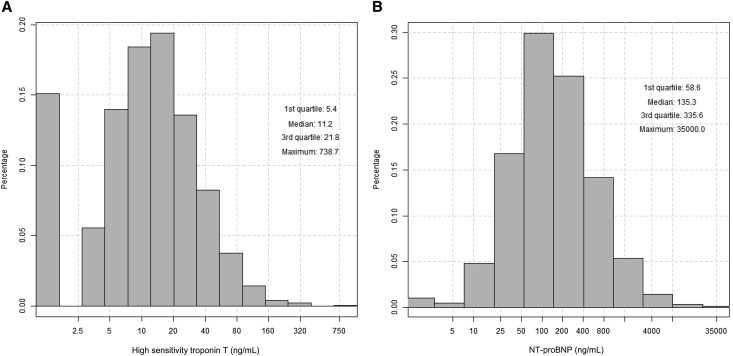
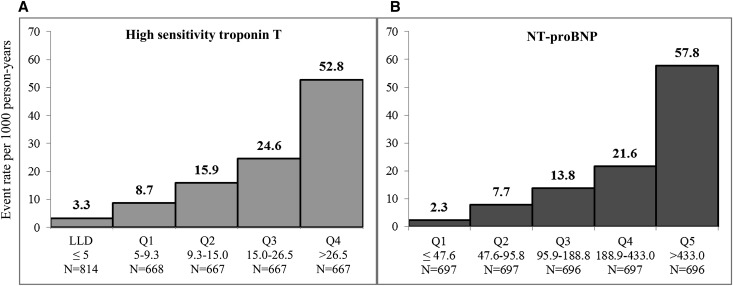
High-sensitivity troponin T (hsTnT) and N-terminal pro-B-type natriuretic peptide (NT-proBNP) strongly predict heart failure (HF) in the general population. However, the interpretation of levels of these biomarkers as predictors of HF is uncertain among patients with CKD. Here, we investigated whether hsTnT and NT-proBNP are associated with incident HF among patients with CKD. In a prospective cohort analysis, we studied 3483 people with CKD in the Chronic Renal Insufficiency Cohort (CRIC) Study recruited from June of 2003 to August of 2008 who were free of HF at baseline. We used Cox regression to examine the association of baseline levels of hsTnT and NT-proBNP with incident HF after adjustment for demographic factors, traditional cardiovascular risk factors, markers of kidney disease, pertinent medication use, and mineral metabolism markers. At baseline, hsTnT levels ranged from ≤5.0 to 738.7 pg/ml, and NT-proBNP levels ranged from ≤5 to 35,000 pg/ml. Compared with those who had undetectable hsTnT, participants in the highest quartile (>26.5 pg/ml) had a significantly higher rate of HF (hazard ratio, 4.77; 95% confidence interval, 2.49 to 9.14). Similarly, compared with those in the lowest NT-proBNP quintile (<47.6 pg/ml), participants in the highest quintile (>433.0 pg/ml) experienced a substantially higher rate of HF (hazard ratio, 9.57; 95% confidence interval, 4.40 to 20.83) [corrected]. In conclusion, hsTnT and NT-proBNP were strongly associated with incident HF among a diverse cohort of individuals with mild to severe CKD. Elevations in these biomarkers may indicate subclinical changes in volume and myocardial stress that subsequently contribute to clinical HF.
Keywords: cardiovascular disease; heart failure; kidney disease.
Copyright © 2015 by the American Society of Nephrology.
Figures
Similar articles
-
Association of Cardiac Biomarkers With the Kansas City Cardiomyopathy Questionnaire in Patients With Chronic Kidney Disease Without Heart Failure.J Am Heart Assoc. 2020 Jul 7;9(13):e014385. doi: 10.1161/JAHA.119.014385. Epub 2020 Jun 24. J Am Heart Assoc. 2020. PMID: 32578483 Free PMC article.
-
Change in Cardiac Biomarkers and Risk of Incident Heart Failure and Atrial Fibrillation in CKD: The Chronic Renal Insufficiency Cohort (CRIC) Study.Am J Kidney Dis. 2021 Jun;77(6):907-919. doi: 10.1053/j.ajkd.2020.09.021. Epub 2020 Dec 9. Am J Kidney Dis. 2021. PMID: 33309861 Free PMC article.
-
Upper Reference Limits for High-Sensitivity Cardiac Troponin T and N-Terminal Fragment of the Prohormone Brain Natriuretic Peptide in Patients With CKD.Am J Kidney Dis. 2022 Mar;79(3):383-392. doi: 10.1053/j.ajkd.2021.06.017. Epub 2021 Jul 19. Am J Kidney Dis. 2022. PMID: 34293394 Free PMC article.
-
[Laboratory Aspects of Using the Results of NT-Probnp Concentration Immunochemical Determination in the Management of Patients With Heart Failure: Support For Clinical Decision-Making].Kardiologiia. 2024 Aug 31;64(8):68-78. doi: 10.18087/cardio.2024.8.n2720. Kardiologiia. 2024. PMID: 39262356 Review. Russian.
-
Applications of cardiac biomarkers in chronic kidney disease.Curr Opin Nephrol Hypertens. 2022 Nov 1;31(6):534-540. doi: 10.1097/MNH.0000000000000829. Epub 2022 Aug 4. Curr Opin Nephrol Hypertens. 2022. PMID: 36004954 Free PMC article. Review.
Cited by
-
Plasma B-type natriuretic peptide is independently associated with cardiovascular events and mortality in patients with chronic kidney disease.Sci Rep. 2024 Jul 17;14(1):16542. doi: 10.1038/s41598-024-67529-1. Sci Rep. 2024. PMID: 39019977 Free PMC article.
-
Chronic Renal Insufficiency Cohort Study (CRIC): Overview and Summary of Selected Findings.Clin J Am Soc Nephrol. 2015 Nov 6;10(11):2073-83. doi: 10.2215/CJN.04260415. Epub 2015 Aug 11. Clin J Am Soc Nephrol. 2015. PMID: 26265715 Free PMC article. Review.
-
Improving the prognosis of patients with severely decreased glomerular filtration rate (CKD G4+): conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference.Kidney Int. 2018 Jun;93(6):1281-1292. doi: 10.1016/j.kint.2018.02.006. Epub 2018 Apr 12. Kidney Int. 2018. PMID: 29656903 Free PMC article.
-
New and Emerging Biomarkers in Chronic Kidney Disease.Biomedicines. 2025 Jun 10;13(6):1423. doi: 10.3390/biomedicines13061423. Biomedicines. 2025. PMID: 40564142 Free PMC article. Review.
-
Heart Failure Increases the Risk of Adverse Renal Outcomes in Patients With Normal Kidney Function.Circ Heart Fail. 2017 Aug;10(8):e003825. doi: 10.1161/CIRCHEARTFAILURE.116.003825. Circ Heart Fail. 2017. PMID: 28765150 Free PMC article.
References
-
- Kottgen A, Russell SD, Loehr LR, Crainiceanu CM, Rosamond WD, Chang PP, Chambless LE, Coresh J: Reduced kidney function as a risk factor for incident heart failure: The atherosclerosis risk in communities (ARIC) study. J Am Soc Nephrol 18: 1307–1315, 2007 - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004 - PubMed
-
- Yamada S, Ishii H, Takahashi H, Aoyama T, Morita Y, Kasuga H, Kimura K, Ito Y, Takahashi R, Toriyama T, Yasuda Y, Hayashi M, Kamiya H, Yuzawa Y, Maruyama S, Matsuo S, Matsubara T, Murohara T: Prognostic value of reduced left ventricular ejection fraction at start of hemodialysis therapy on cardiovascular and all-cause mortality in end-stage renal disease patients. Clin J Am Soc Nephrol 5: 1793–1798, 2010 - PMC - PubMed
-
- Saunders JT, Nambi V, de Lemos JA, Chambless LE, Virani SS, Boerwinkle E, Hoogeveen RC, Liu X, Astor BC, Mosley TH, Folsom AR, Heiss G, Coresh J, Ballantyne CM: Cardiac troponin T measured by a highly sensitive assay predicts coronary heart disease, heart failure, and mortality in the Atherosclerosis Risk in Communities Study. Circulation 123: 1367–1376, 2011 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 DK072231/DK/NIDDK NIH HHS/United States
- K24 DK002651/DK/NIDDK NIH HHS/United States
- K23-DK088865/DK/NIDDK NIH HHS/United States
- K01 DK092353/DK/NIDDK NIH HHS/United States
- U01-DK060984/DK/NIDDK NIH HHS/United States
- UL1-TR000433/TR/NCATS NIH HHS/United States
- UL1-RR029879/RR/NCRR NIH HHS/United States
- U01-DK061021/DK/NIDDK NIH HHS/United States
- P30-GM103337/GM/NIGMS NIH HHS/United States
- M01 RR-16500/RR/NCRR NIH HHS/United States
- UL1 RR029879/RR/NCRR NIH HHS/United States
- U01 DK061028/DK/NIDDK NIH HHS/United States
- UL1 TR000433/TR/NCATS NIH HHS/United States
- U01-DK060980/DK/NIDDK NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- U01 DK061021/DK/NIDDK NIH HHS/United States
- UL1 RR-024131/RR/NCRR NIH HHS/United States
- P30 GM103337/GM/NIGMS NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- K01-DK092353/DK/NIDDK NIH HHS/United States
- U01 DK060963/DK/NIDDK NIH HHS/United States
- U01-DK061022/DK/NIDDK NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- K24-DK02651/DK/NIDDK NIH HHS/United States
- U01-DK060990/DK/NIDDK NIH HHS/United States
- U01 DK061022/DK/NIDDK NIH HHS/United States
- R01 DK103612/DK/NIDDK NIH HHS/United States
- UL1-TR000003/TR/NCATS NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- UL1-TR000439/TR/NCATS NIH HHS/United States
- R01 DK066488/DK/NIDDK NIH HHS/United States
- 1DK066488/DK/NIDDK NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- K23 DK088865/DK/NIDDK NIH HHS/United States
- U01-DK060902/DK/NIDDK NIH HHS/United States
- R01 DK081374/DK/NIDDK NIH HHS/United States
- U01-DK060963/DK/NIDDK NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
- U01-DK061028/DK/NIDDK NIH HHS/United States
- K24 DK093723/DK/NIDDK NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- UL1-TR-000424/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
