

CKD and hypertension during long-term follow-up in children and adolescents previously treated with extracorporeal membrane oxygenation
- PMID: 25278545
- PMCID: PMC4255400
- DOI: 10.2215/CJN.02890314
CKD and hypertension during long-term follow-up in children and adolescents previously treated with extracorporeal membrane oxygenation
Abstract
Background and objectives: Many children receiving extracorporeal membrane oxygenation develop AKI. If AKI leads to permanent nephron loss, it may increase the risk of developing CKD. The prevalence of CKD and hypertension and its predictive factors during long-term follow-up of children and adolescents previously treated with neonatal extracorporeal membrane oxygenation were determined.
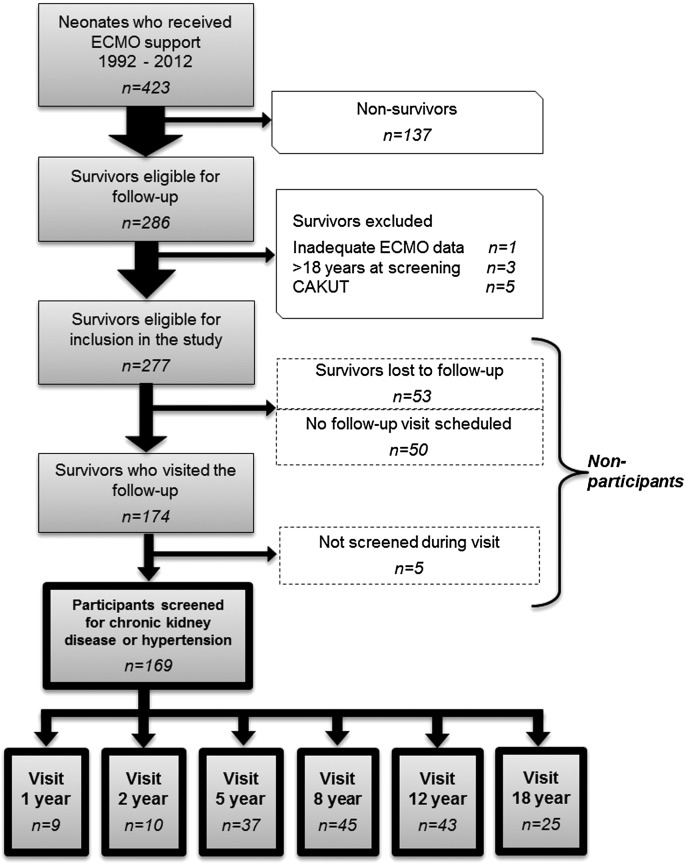
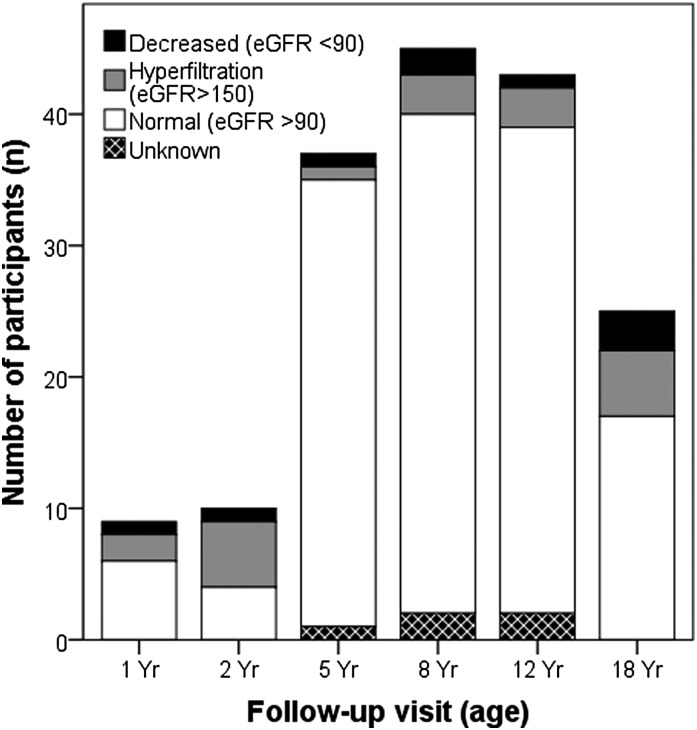
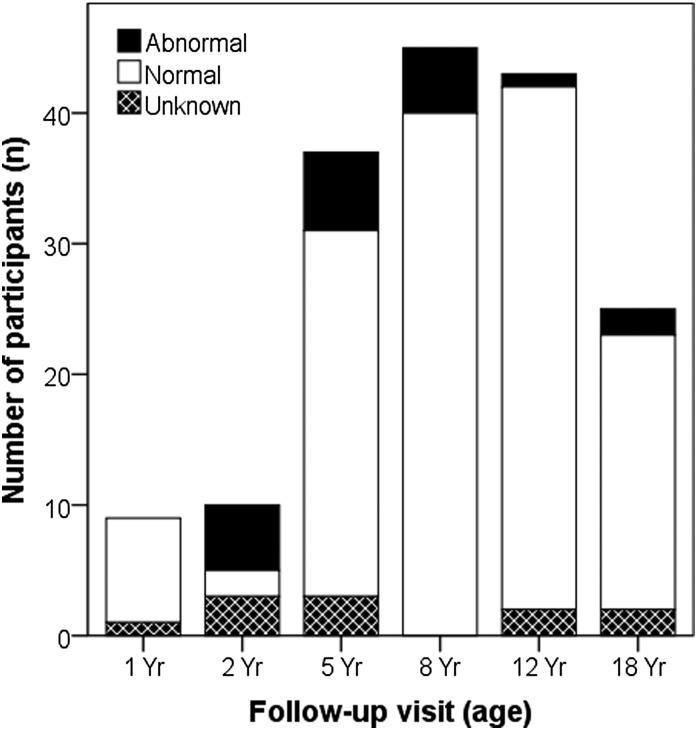
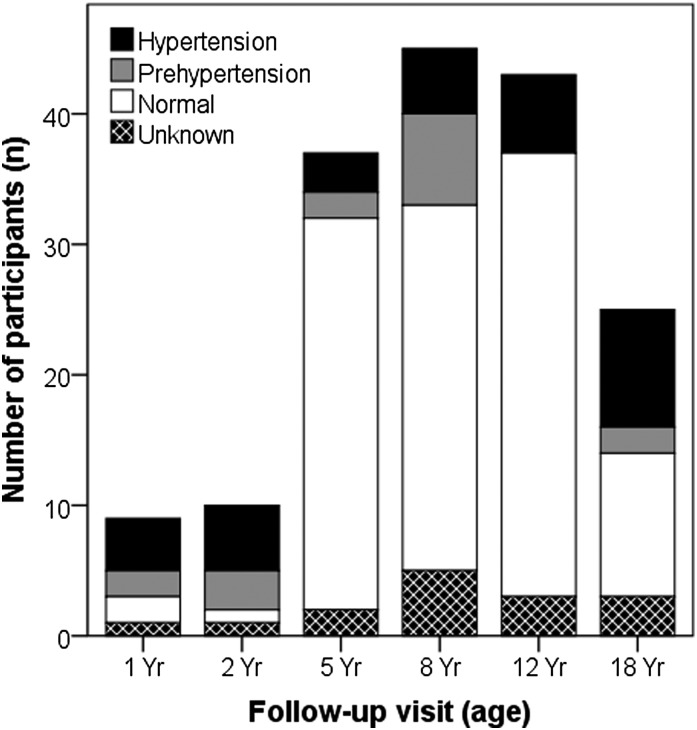
Design, setting, participants, & measurements: Between November of 2010 and February of 2014, neonatal survivors of extracorporeal membrane oxygenation who visited the prospective follow-up program at 1, 2, 5, 8, 12, and 18 years of age were screened for CKD and hypertension (BP≥95th percentile of reference values). CKD was suspected in children with either an eGFR<90 ml/min per 1.73 m(2) or proteinuria (urinary protein-to-creatinine ratio >0.50 for children ages ≤24 months and >0.20 at >24 months). The RIFLE classification (risk, injury, or failure as 150%, 200%, or 300% of serum creatinine reference values) was used to define AKI during extracorporeal membrane oxygenation without preemptive hemofiltration.
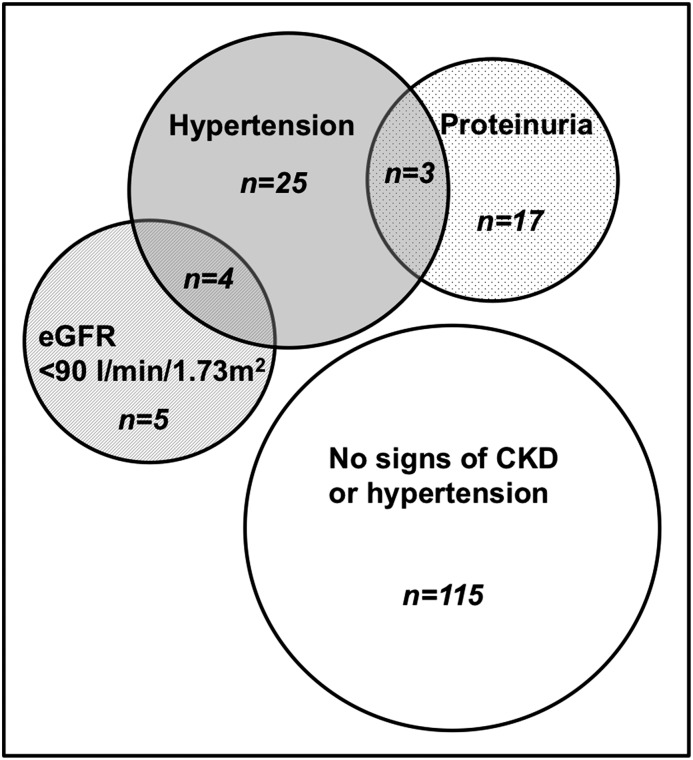
Results: Median follow-up of 169 screened participants was 8.2 years (interquartile range=5.2-12.1 years). Nine children had a lower eGFR, but all rates were >60 ml/min per 1.73 m(2). Proteinuria was observed in 20 children (median=0.26 mg protein/mg creatinine; interquartile range=0.23-0.32 mg protein/mg creatinine), and 32 children had hypertension. Only history of AKI was associated with CKD (P=0.004). Children with RIFLE scores injury and failure had 4.3 times higher odds of CKD signs or hypertension than those without AKI (95% confidence interval, 1.6 to 12.1; P=0.004).
Conclusions: Altogether, 54 participants (32%) had at least one sign of CKD and/or hypertension. However, most values were marginally abnormal, with no immediate consequences for clinical care. Nevertheless, a prevalence of 32% clearly indicates that survivors of neonatal extracorporeal membrane oxygenation, especially those with AKI, are at risk of a more rapid decline of kidney function with increasing age. Therefore, screening for CKD development in adulthood is recommended.
Keywords: CKD; acute renal; children; clinical nephrology; epidemiology and outcomes; failure.
Copyright © 2014 by the American Society of Nephrology.
Figures
References
-
- Alkandari O, Eddington KA, Hyder A, Gauvin F, Ducruet T, Gottesman R, Phan V, Zappitelli M: Acute kidney injury is an independent risk factor for pediatric intensive care unit mortality, longer length of stay and prolonged mechanical ventilation in critically ill children: A two-center retrospective cohort study. Crit Care 15: R146, 2011 - PMC - PubMed
-
- Bailey D, Phan V, Litalien C, Ducruet T, Mérouani A, Lacroix J, Gauvin F: Risk factors of acute renal failure in critically ill children: A prospective descriptive epidemiological study. Pediatr Crit Care Med 8: 29–35, 2007 - PubMed
-
- Akcan-Arikan A, Zappitelli M, Loftis LL, Washburn KK, Jefferson LS, Goldstein SL: Modified RIFLE criteria in critically ill children with acute kidney injury. Kidney Int 71: 1028–1035, 2007 - PubMed
-
- Schneider J, Khemani R, Grushkin C, Bart R: Serum creatinine as stratified in the RIFLE score for acute kidney injury is associated with mortality and length of stay for children in the pediatric intensive care unit. Crit Care Med 38: 933–939, 2010 - PubMed
-
- Plötz FB, Bouma AB, van Wijk JA, Kneyber MC, Bökenkamp A: Pediatric acute kidney injury in the ICU: An independent evaluation of pRIFLE criteria. Intensive Care Med 34: 1713–1717, 2008 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
