

Laparoscopic natural orifice specimen extraction-colectomy: a systematic review
- PMID: 25278692
- PMCID: PMC4177477
- DOI: 10.3748/wjg.v20.i36.12981
Laparoscopic natural orifice specimen extraction-colectomy: a systematic review
Abstract
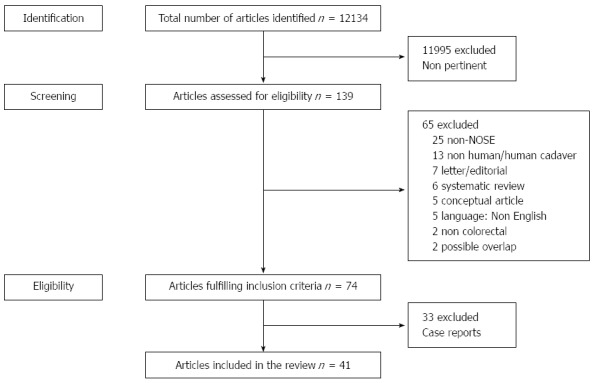
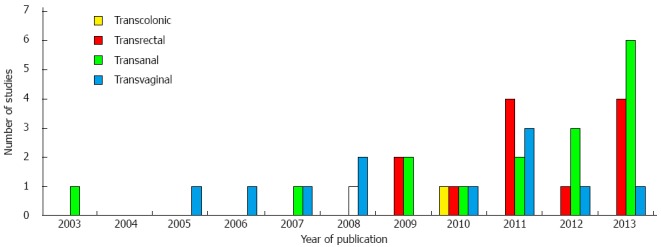
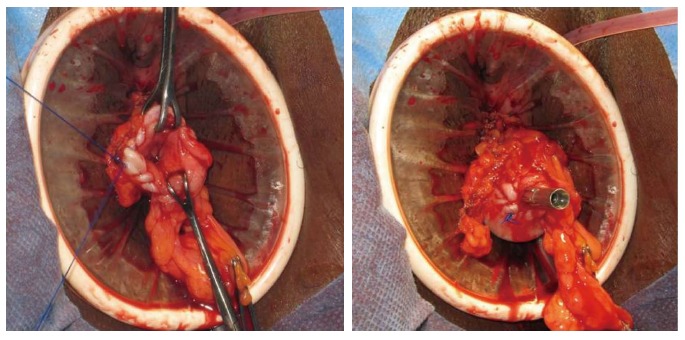
Over the last 20 years, laparoscopic colorectal surgery has shown equal efficacy for benign and malignant colorectal diseases when compared to open surgery. However, a laparoscopic approach reduces postoperative morbidity and shortens hospital stay. In the quest to optimize outcomes after laparoscopic colorectal surgery, reduction of access trauma could be a way to improve recovery. To date, one method to reduce access trauma is natural orifice specimen extraction (NOSE). NOSE aims to reduce access trauma in laparoscopic colorectal surgery. The specimen is delivered via a natural orifice and the anastomosis is created intracorporeally. Different methods are used to extract the specimen and to create a bowel anastomosis. Currently, specimens are delivered transcolonically, transrectally, transanally, or transvaginally. Each of these NOSE-procedures raises specific issues with regard to operative technique and application. The presumed benefits of NOSE-procedures are less pain, lower analgesia requirements, faster recovery, shorter hospital stay, better cosmetic results, and lower incisional hernia rates. Avoidance of extraction site laparotomy is the most important characteristic of NOSE. Concerns associated with the NOSE-technique include bacterial contamination of the peritoneal cavity, inflammatory response, and postoperative outcomes, including postoperative pain and the functional and oncologic outcomes. These issues need to be studied in prospective randomized controlled trials. The aim of this systematic review is to describe the role of NOSE in minimally invasive colorectal surgery.
Keywords: Colorectal surgery; Gastrointestinal endoscopy; Laparoscopy; Natural orifice specimen extraction; Natural orifice specimen extraction-colectomy; Transanal; Transanal minimally invasive surgery; Transcolonic; Transrectal; Transvaginal.
Figures

References
-
- Laurent C, Leblanc F, Bretagnol F, Capdepont M, Rullier E. Long-term wound advantages of the laparoscopic approach in rectal cancer. Br J Surg. 2008;95:903–908. - PubMed
-
- Alba Mesa F, Amaya Cortijo A, Romero Fernandez JM, Komorowski AL, Sanchez Hurtado MA, Fernandez Ortega E, Sanchez Margallo FM. Transvaginal sigmoid cancer resection: first case with 12 months of follow-up--technique description. J Laparoendosc Adv Surg Tech A. 2012;22:587–590. - PubMed
-
- Allam M, Piskun G, Fogler R. Laparoscopic-assisted abdominoperineal proctosigmoidectomy for rectal prolapse. A new technique. Surg Endosc. 1997;11:150–151. - PubMed
-
- Atallah S, Nassif G, Polavarapu H, deBeche-Adams T, Ouyang J, Albert M, Larach S. Robotic-assisted transanal surgery for total mesorectal excision (RATS-TME): a description of a novel surgical approach with video demonstration. Tech Coloproctol. 2013;17:441–447. - PubMed
-
- Awad ZT. Laparoscopic subtotal colectomy with transrectal extraction of the colon and ileorectal anastomosis. Surg Endosc. 2012;26:869–871. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
