

Minimally invasive surgery for submucosal (subepithelial) tumors of the stomach
- PMID: 25278697
- PMCID: PMC4177482
- DOI: 10.3748/wjg.v20.i36.13035
Minimally invasive surgery for submucosal (subepithelial) tumors of the stomach
Abstract
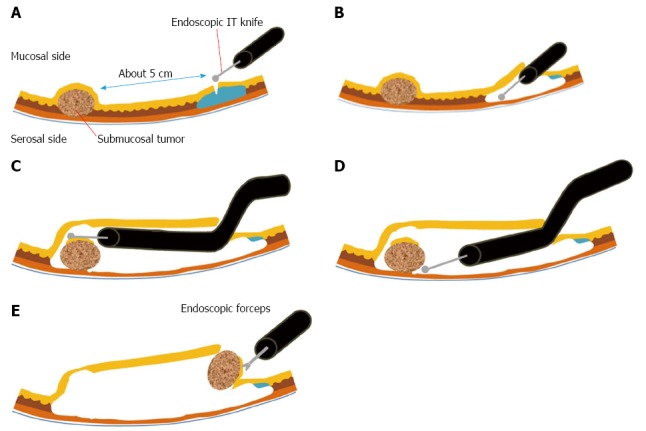
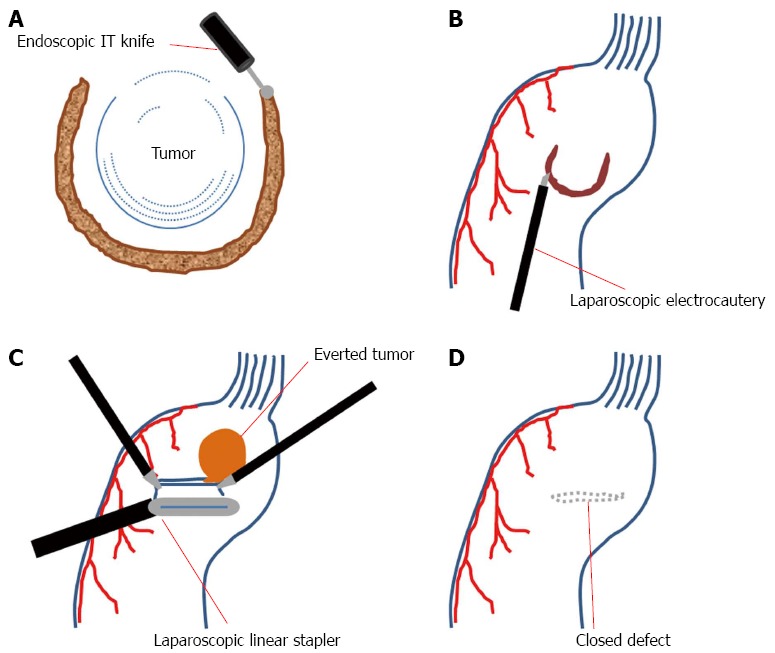
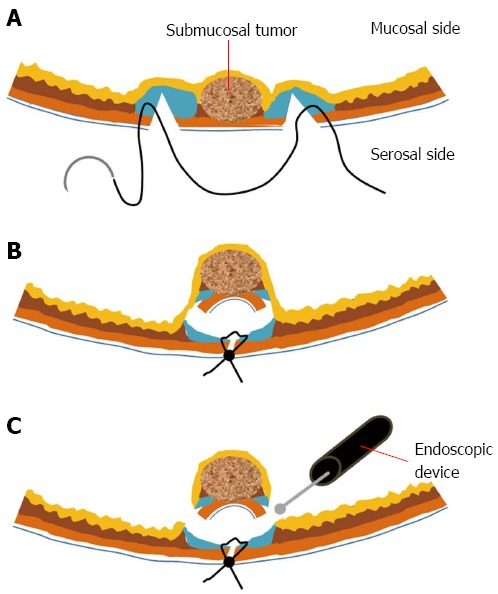
Minimally invasive surgery has become common in the surgical resection of gastrointestinal submucosal tumors (SMTs). The purpose of this article is to review recent trends in minimally invasive surgery for gastric SMTs. Although laparoscopic resection has been main stream of minimally invasive surgery for gastrointestinal SMTs, recent advances in endoscopic procedures now provide various treatment modalities for gastric SMTs. Moreover, investigators have developed several hybrid techniques that include the advantages of both laparoscopic and endoscopic procedure. In addition, several types of reduced port surgeries, modification of conventional laparoscopic procedures, have been recently applied to the surgical resection of SMTs. Meanwhile, robotic surgery for SMTs requires further evidence and improvement.
Keywords: Gastrointestinal tract; Minimally invasive; Submucosal tumor; Surgery.
Figures
References
-
- Dubois F, Berthelot G, Levard H. [Cholecystectomy by coelioscopy] Presse Med. 1989;18:980–982. - PubMed
-
- Hwang SH, Park do J, Kim YH, Lee KH, Lee HS, Kim HH, Lee HJ, Yang HK, Lee KU. Laparoscopic surgery for submucosal tumors located at the esophagogastric junction and the prepylorus. Surg Endosc. 2009;23:1980–1987. - PubMed
-
- Tsushimi T, Matsui N, Kurazumi H, Takemoto Y, Oka K, Seyama A, Morita T. Laparoscopic resection of an ileal lipoma: Report of a case. Surg Today. 2006;36:1007–1011. - PubMed
-
- Lin MW, Chen KH, Lin HF, Chen HA, Wu JM, Huang SH. Laparoscopy-assisted resection of ileoileal intussusception caused by intestinal lipoma. J Laparoendosc Adv Surg Tech A. 2007;17:789–792. - PubMed
-
- Ako E, Morisaki T, Hasegawa T, Hirakawa T, Tachimori A, Nakazawa K, Yamagata S, Kanehara I, Nishimura S, Taenaka N. Laparoscopic resection of ileal lipoma diagnosed by multidetector-row computed tomography. Surg Laparosc Endosc Percutan Tech. 2010;20:e226–e229. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
