

Different patterns of punctate white matter lesions in serially scanned preterm infants
- PMID: 25279755
- PMCID: PMC4184838
- DOI: 10.1371/journal.pone.0108904
Different patterns of punctate white matter lesions in serially scanned preterm infants
Erratum in
- PLoS One. 2014;9(11):e114704
Abstract
Background and purpose: With the increased use of MRI in preterm infants, punctate white matter lesions (PWML) are more often recognized. The aim of this study was to describe the incidence and characteristics of these lesions as well as short-term outcome in a cohort of serially scanned preterm infants, using both conventional imaging, diffusion (DWI) and susceptibility (SWI) weighted imaging.
Materials and methods: 112 preterm infants with 2 MRIs in the neonatal period, with evidence of punctate white matter lesions, were included. Appearance, lesion load, location, and abnormalities on DWI and SWI were scored and outcome data were collected.
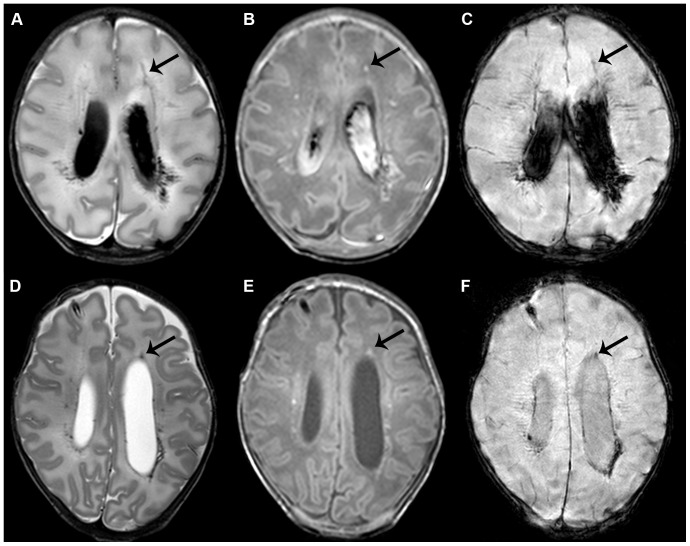
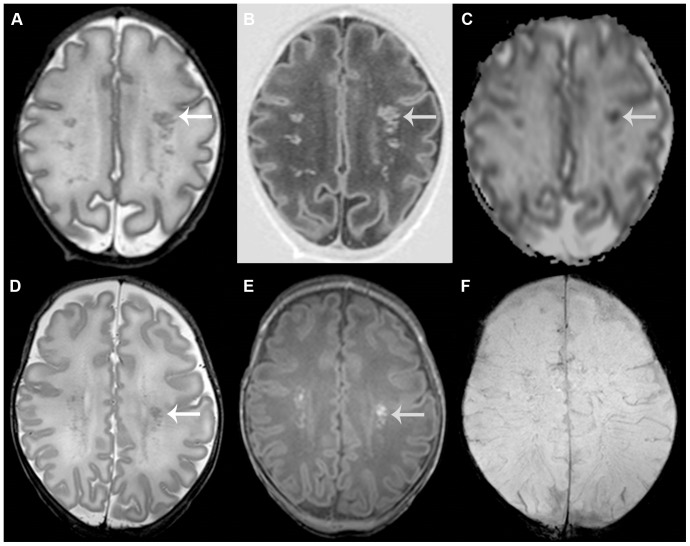
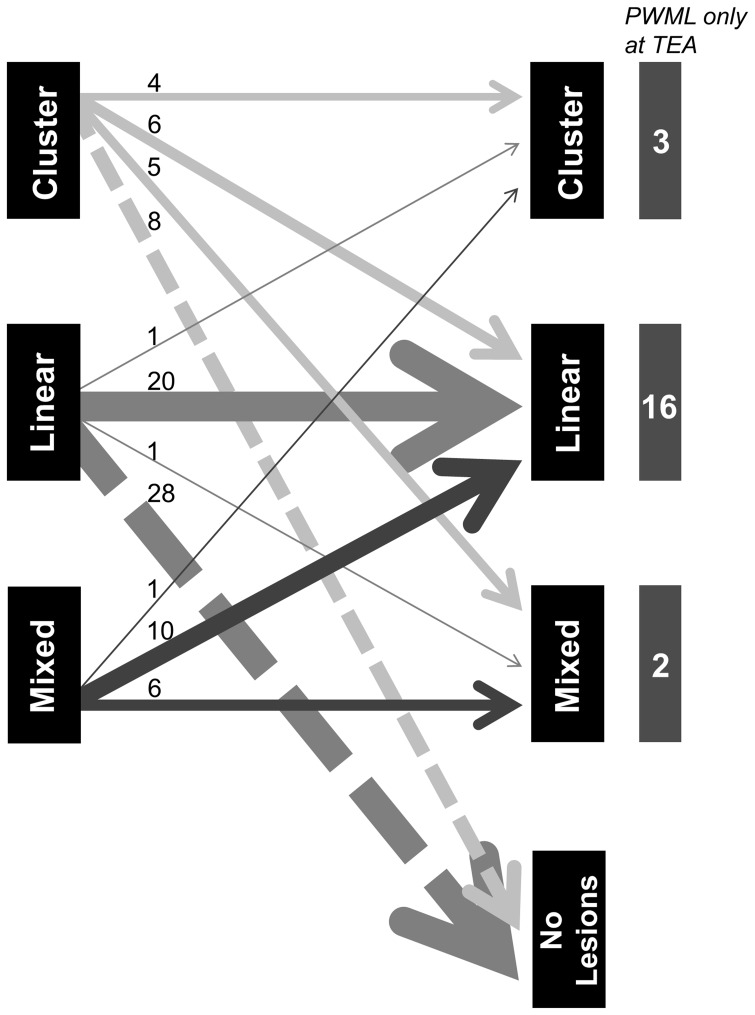
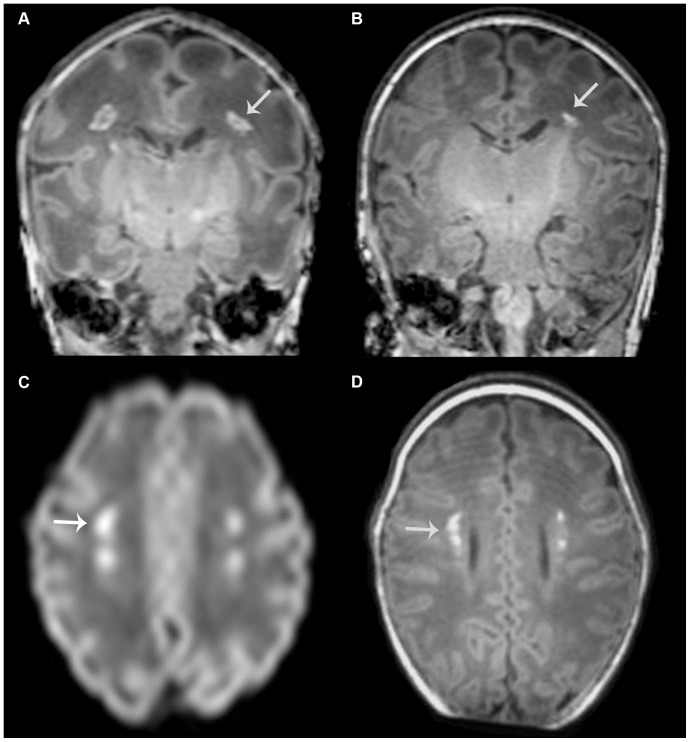
Results: Different patterns of punctate white matter lesions did appear: a linear appearance associated with signal loss on SWI, and a cluster appearance associated with restricted diffusion on DWI on the first MRI. Cluster and mixed lesions on the first scan changed in appearance in over 50% on the second scan, whereas linear lesions generally kept their appearance. Lesions were only visible on the early scan in 33%, and were only seen at term equivalent age in 20%. Nine infants developed cerebral palsy, due to additional overt white matter lesions in six.
Conclusion: Two patterns of punctate white matter lesions were identified: one with loss of signal on SWI in a linear appearance, and the other with DWI lesions with restricted diffusion in a cluster appearance. These different patterns are suggestive of a difference in underlying pathophysiology. To reliably classify PWML in the preterm infant in either pattern, an early MRI with DWI and SWI sequences is required.
Conflict of interest statement
Figures
References
-
- Maalouf EF, Duggan PJ, Counsell SJ, Rutherford MA, Cowan F, et al. (2001) Comparison of findings on cranial ultrasound and magnetic resonance imaging in preterm infants. Pediatrics 107: 719–727. - PubMed
-
- de Bruine FT, van den Berg-Huysmans AA, Leijser LM, Rijken M, Steggerda SJ, et al. (2011) Clinical implications of MR imaging findings in the white matter in very preterm infants: a 2-year follow-up study. Radiology 261: 899–906. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
