

Respiratory inductance plethysmography calibration for pediatric upper airway obstruction: an animal model
- PMID: 25279987
- PMCID: PMC4268304
- DOI: 10.1038/pr.2014.144
Respiratory inductance plethysmography calibration for pediatric upper airway obstruction: an animal model
Abstract
Background: We sought to determine optimal methods of respiratory inductance plethysmography (RIP) flow calibration for application to pediatric postextubation upper airway obstruction.
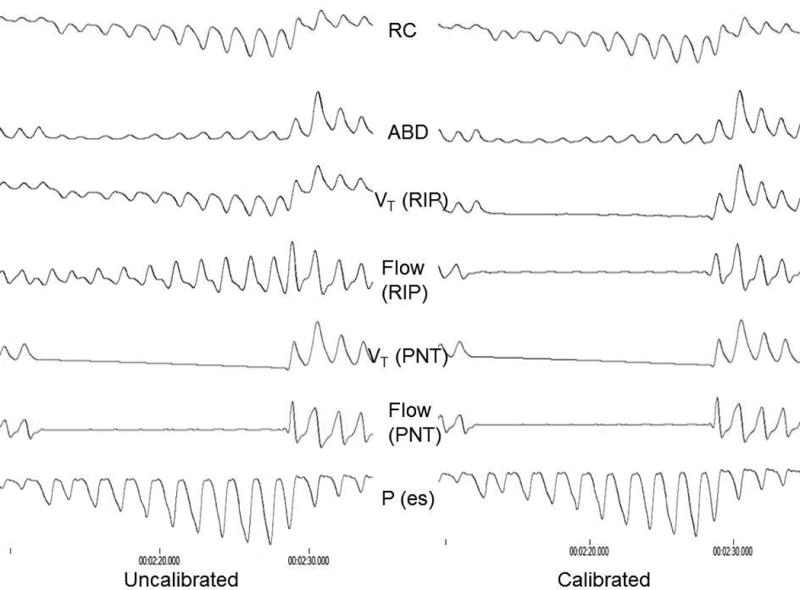
Methods: We measured RIP, spirometry, and esophageal manometry in spontaneously breathing, intubated Rhesus monkeys with increasing inspiratory resistance. RIP calibration was based on: ΔµV(ao) ≈ M[ΔµV(RC) + K(ΔµV(AB))] where K establishes the relationship between the uncalibrated rib cage (ΔµV(RC)) and abdominal (ΔµV(AB)) RIP signals. We calculated K during (i) isovolume maneuvers during a negative inspiratory force (NIF), (ii) quantitative diagnostic calibration (QDC) during (a) tidal breathing, (b) continuous positive airway pressure (CPAP), and (c) increasing degrees of upper airway obstruction (UAO). We compared the calibrated RIP flow waveform to spirometry quantitatively and qualitatively.
Results: Isovolume calibrated RIP flow tracings were more accurate (against spirometry) both quantitatively and qualitatively than those from QDC (P < 0.0001), with bigger differences as UAO worsened. Isovolume calibration yielded nearly identical clinical interpretation of inspiratory flow limitation as spirometry.
Conclusion: In an animal model of pediatric UAO, isovolume calibrated RIP flow tracings are accurate against spirometry. QDC during tidal breathing yields poor RIP flow calibration, particularly as UAO worsens. Routine use of a NIF maneuver before extubation affords the opportunity to use RIP to study postextubation UAO in children.
Conflict of interest statement
There are no conflicts of interest for any of the authors.
Figures





References
-
- Argent AC, Newth CJ, Klein M. The mechanics of breathing in children with acute severe croup. Intensive Care Med. 2008;34:324–32. - PubMed
-
- Newth CJ, Levison H, Bryan AC. The respiratory status of children with croup. J Pediatr. 1972;81:1068–73. - PubMed
-
- Argent AC, Hatherill M, Newth CJ, Klein M. The effect of epinephrine by nebulization on measures of airway obstruction in patients with acute severe croup. Intensive Care Med. 2008;34:138–47. 2008. - PubMed
-
- Kaplan V, Zhang JN, Russi EW, Bloch KE. Detection of inspiratory flow limitation during sleep by computer assisted respiratory inductive plethysmography. Eur Respir J. 2000;15:570–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
