

Association between molecular subtypes of colorectal cancer and patient survival
- PMID: 25280443
- PMCID: PMC4274235
- DOI: 10.1053/j.gastro.2014.09.038
Association between molecular subtypes of colorectal cancer and patient survival
Abstract
Background and aims: Colorectal cancer (CRC) is a heterogeneous disease that can develop via several pathways. Different CRC subtypes, identified based on tumor markers, have been proposed to reflect these pathways. We evaluated the significance of these previously proposed classifications to survival.
Methods: Participants in the population-based Seattle Colon Cancer Family Registry were diagnosed with invasive CRC from 1998 through 2007 in western Washington State (N = 2706), and followed for survival through 2012. Tumor samples were collected from 2050 participants and classified into 5 subtypes based on combinations of tumor markers: type 1 (microsatellite instability [MSI]-high, CpG island methylator phenotype [CIMP] -positive, positive for BRAF mutation, negative for KRAS mutation); type 2 (microsatellite stable [MSS] or MSI-low, CIMP-positive, positive for BRAF mutation, negative for KRAS mutation); type 3 (MSS or MSI low, non-CIMP, negative for BRAF mutation, positive for KRAS mutation); type 4 (MSS or MSI-low, non-CIMP, negative for mutations in BRAF and KRAS); and type 5 (MSI-high, non-CIMP, negative for mutations in BRAF and KRAS). Multiple imputation was used to impute tumor markers for those missing data on 1-3 markers. We used Cox regression to estimate hazard ratios (HR) and 95% confidence intervals (CI) for associations of subtypes with disease-specific and overall mortality, adjusting for age, sex, body mass, diagnosis year, and smoking history.
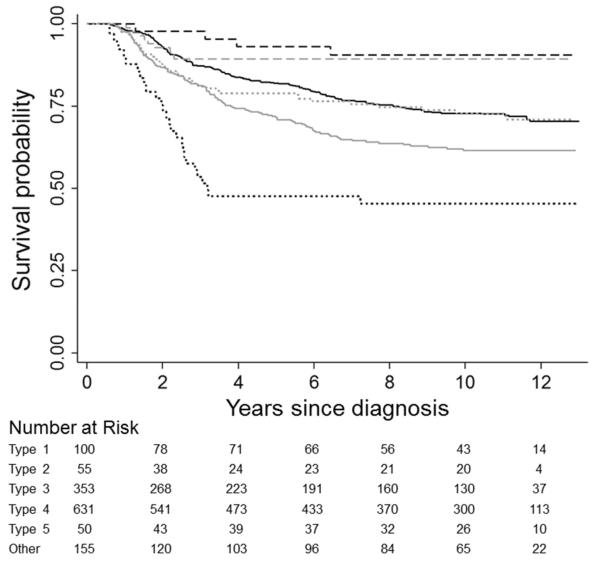
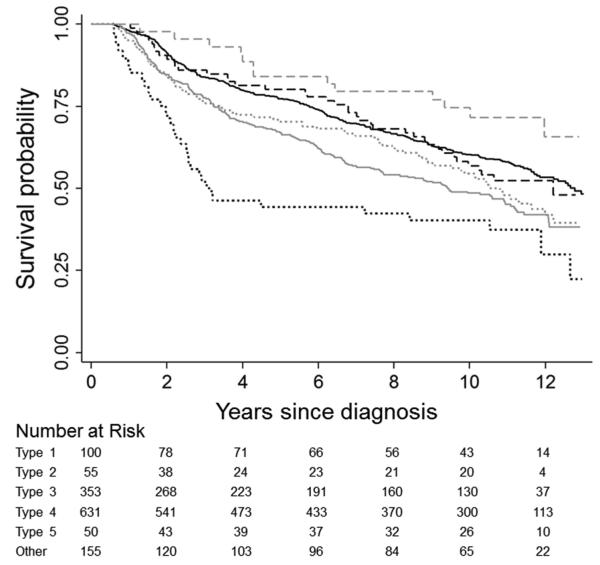
Results: Compared with participants with type 4 tumors (the most predominant), participants with type 2 tumors had the highest disease-specific mortality (HR = 2.20, 95% CI: 1.47-3.31); subjects with type 3 tumors also had higher disease-specific mortality (HR = 1.32, 95% CI: 1.07-1.63). Subjects with type 5 tumors had the lowest disease-specific mortality (HR = 0.30, 95% CI: 0.14-0.66). Associations with overall mortality were similar to those with disease-specific mortality.
Conclusions: Based on a large, population-based study, CRC subtypes, defined by proposed etiologic pathways, are associated with marked differences in survival. These findings indicate the clinical importance of studies into the molecular heterogeneity of CRC.
Keywords: Methylation; Oncogene; Prognostic Factor; Serrated Colorectal Cancer.
Copyright © 2015 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Molecular subtyping of colorectal cancer: time to explore both intertumoral and intratumoral heterogeneity to evaluate patient outcome.Gastroenterology. 2015 Jan;148(1):10-3. doi: 10.1053/j.gastro.2014.11.024. Epub 2014 Nov 22. Gastroenterology. 2015. PMID: 25451650 Free PMC article. No abstract available.
References
-
- Jass JR. Classification of colorectal cancer based on correlation of clinical, morphological and molecular features. Histopathology. 2007;50:113–30. - PubMed
-
- Leggett B, Whitehall V. Role of the serrated pathway in colorectal cancer pathogenesis. Gastroenterology. 2010;138:2088–100. - PubMed
-
- Samowitz WS, Curtin K, Schaffer D, et al. Relationship of Ki-ras mutations in colon cancers to tumor location, stage, and survival: A population-based study. Cancer Epidemiology Biomarkers & Prevention. 2000;9:1193–1197. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 CA076366/CA/NCI NIH HHS/United States
- R01 CA118699/CA/NCI NIH HHS/United States
- R01CA118699/CA/NCI NIH HHS/United States
- R01CA107333/CA/NCI NIH HHS/United States
- R01 CA107333/CA/NCI NIH HHS/United States
- K05CA142885/CA/NCI NIH HHS/United States
- U24 CA074794/CA/NCI NIH HHS/United States
- K07CA172298/CA/NCI NIH HHS/United States
- U01 CA074794/CA/NCI NIH HHS/United States
- KL2TR000421/TR/NCATS NIH HHS/United States
- R01CA076366/CA/NCI NIH HHS/United States
- KL2 TR000421/TR/NCATS NIH HHS/United States
- K07 CA172298/CA/NCI NIH HHS/United States
- K05 CA152715/CA/NCI NIH HHS/United States
- UM1 CA167551/CA/NCI NIH HHS/United States
- K05 CA142885/CA/NCI NIH HHS/United States
- U01CA74794/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
