

Pharmacy refill adherence outperforms self-reported methods in predicting HIV therapy outcome in resource-limited settings
- PMID: 25280535
- PMCID: PMC4194413
- DOI: 10.1186/1471-2458-14-1035
Pharmacy refill adherence outperforms self-reported methods in predicting HIV therapy outcome in resource-limited settings
Abstract
Background: Optimal adherence to antiretroviral therapy is critical to prevent HIV drug resistance (HIVDR) epidemic. The objective of the study was to investigate the best performing adherence assessment method for predicting virological failure in resource-limited settings (RLS).
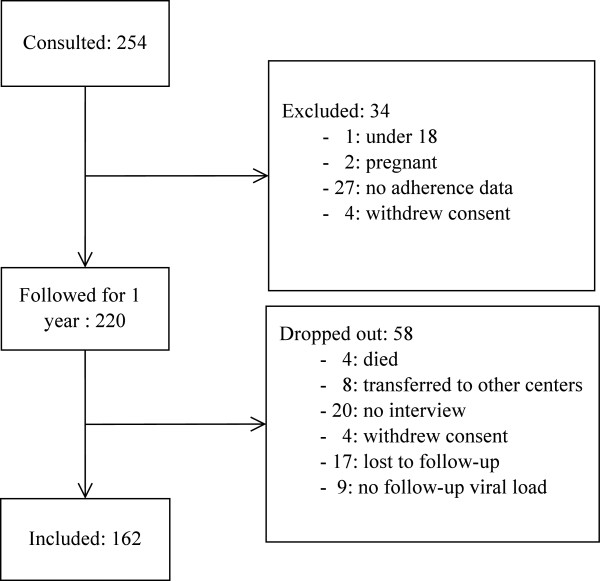
Method: This study was a single-centre prospective cohort, enrolling 220 HIV-infected adult patients attending an HIV/AIDS Care and Treatment Centre in Dar es Salaam, Tanzania, in 2010. Pharmacy refill, self-report (via visual analog scale [VAS] and the Swiss HIV Cohort study-adherence questionnaire), pill count, and appointment keeping adherence measurements were taken. Univariate logistic regression (LR) was done to explore a cut-off that gives a better trade-off between sensitivity and specificity, and a higher area under the curve (AUC) based on receiver operating characteristic curve in predicting virological failure. Additionally, the adherence models were evaluated by fitting multivariate LR with stepwise functions, decision trees, and random forests models, assessing 10-fold multiple cross validation (MCV). Patient factors associated with virological failure were determined using LR.
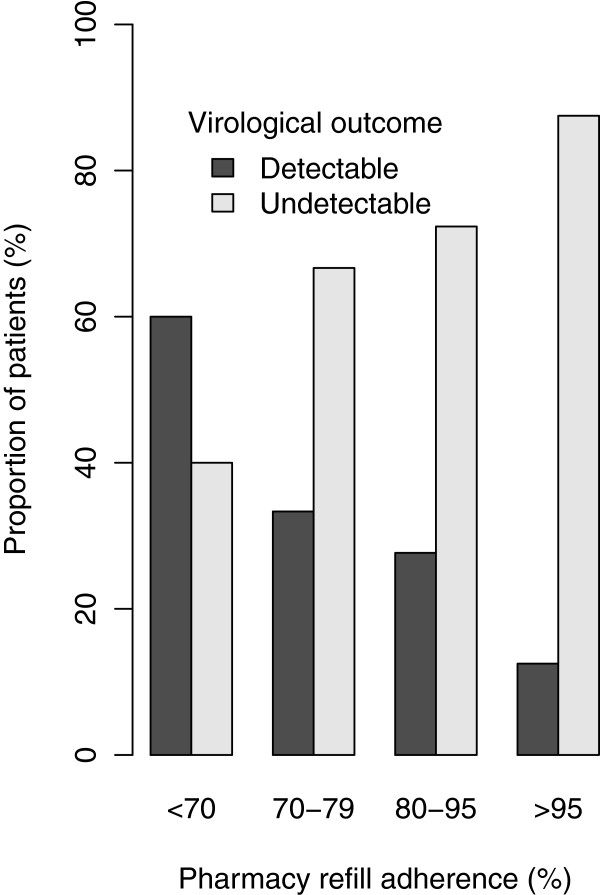
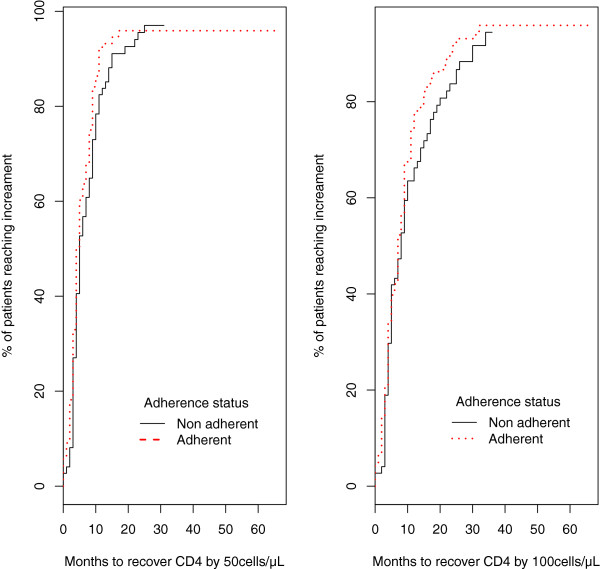
Results: Viral load measurements at baseline and one year after recruitment were available for 162 patients, of whom 55 (34%) had detectable viral load and 17 (10.5%) had immunological failure at one year after recruitment. The optimal cut-off points significantly predictive of virological failure were 95%, 80%, 95% and 90% for VAS, appointment keeping, pharmacy refill, and pill count adherence respectively. The AUC for these methods ranged from 0.52 to 0.61, with pharmacy refill giving the best performance at AUC 0.61. Multivariate logistic regression with boost stepwise MCV had higher AUC (0.64) compared to all univariate adherence models, except pharmacy refill adherence univariate model, which was comparable to the multivariate model (AUC = 0.64). Decision trees and random forests models were inferior to boost stepwise model. Pharmacy refill adherence (<95%) emerged as the best method for predicting virological failure. Other significant predictors in multivariate LR were having a baseline CD4 T lymphocytes count < 200 cells/μl, being unable to recall the diagnosis date, and a higher weight.
Conclusion: Pharmacy refill has the potential to predict virological failure and to identify patients to be considered for viral load monitoring and HIVDR testing in RLS.
Figures
References
-
- Chaiwarith R, Wachirakaphan C, Kotarathititum W, Praparatanaphan J, Sirisanthana T, Supparatpinyo K. Sensitivity and specificity of using CD4+ measurement and clinical evaluation to determine antiretroviral treatment failure in Thailand. Int J Infect Dis. 2007;11:413–416. doi: 10.1016/j.ijid.2006.11.003. - DOI - PubMed
-
- Rawizza HE, Chaplin B, Meloni ST, Eisen G, Rao T, Sankalé J-L, Dieng-Sarr A, Agbaji O, Onwujekwe DI, Gashau W, Nkado R, Ekong E, Okonkwo P, Murphy RL, Kanki PJ. Immunologic criteria are poor predictors of virologic outcome: implications for HIV treatment monitoring in resource-limited settings. Clin Infect Dis. 2011;53:1283–1290. doi: 10.1093/cid/cir729. - DOI - PMC - PubMed
-
- De Luca A, Marazzi MC, Mancinelli S, Ceffa S, Altan AMD, Buonomo E, Prosperi MCF, Pedruzzi B, Noorjehan AM, Scarcella P, Liotta G, Palombi L. Prognostic value of virological and immunological responses after 6 months of antiretroviral treatment in adults with HIV-1 infection in sub-Saharan Africa. J Acquir Immune Defic Syndr. 2012;59:236–244. doi: 10.1097/QAI.0b013e31824276e9. - DOI - PubMed
-
- Chi BH, Cantrell RA, Zulu I, Mulenga LB, Levy JW, Tambatamba BC, Reid S, Mwango A, Mwinga A, Bulterys M, Saag MS, Stringer JSA. Adherence to first-line antiretroviral therapy affects non-virologic outcomes among patients on treatment for more than 12 months in Lusaka, Zambia. Int J Epidemiol. 2009;38:746–756. doi: 10.1093/ije/dyp004. - DOI - PMC - PubMed
Pre-publication history
-
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/14/1035/prepub
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
