

A novel procedure for transtracheal resection for recurrent thyroid cancer involving a trachea and esophagus
- PMID: 25280536
- PMCID: PMC4197303
- DOI: 10.1186/1477-7819-12-303
A novel procedure for transtracheal resection for recurrent thyroid cancer involving a trachea and esophagus
Abstract
Background: Surgery remains the main treatment for locally advanced thyroid cancers invading the trachea, esophagus, and recurrent laryngeal nerve. However, extensive resection of such tumors can sometimes involve difficulties and may result in the deterioration of the patient's quality of life. The surgeon should consider not only the patient's prognosis but also the preservation of postoperative function.
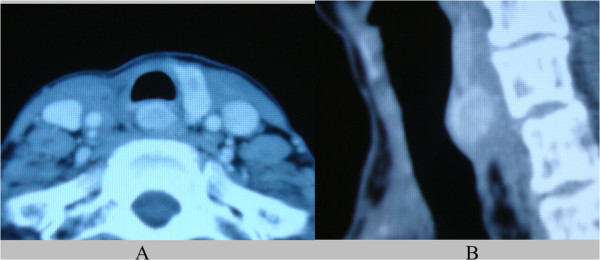
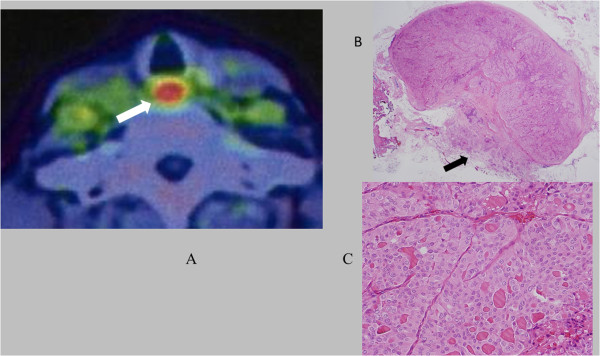
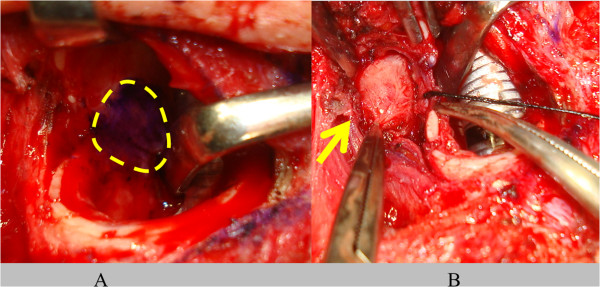
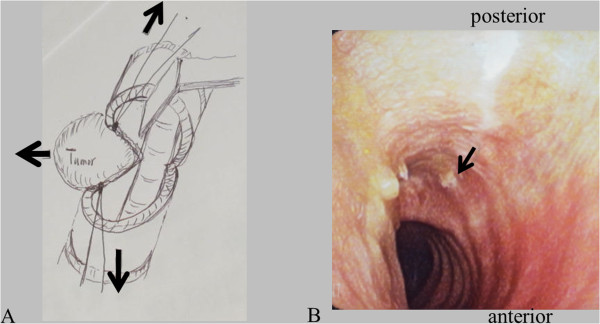
Methods: This report describes a minimally invasive surgical procedure for recurrent poorly differentiated papillary thyroid carcinoma involving the trachea and esophagus. To decrease the potential for recurrent laryngeal nerve injuries and to preserve both the tracheal and esophageal blood supply, we adapted a transtracheal approach; the recurrent tumor was safely and completely removed without causing a dysfunction. After a tracheotomy to the right, the tumor was easily detected through the tracheostoma and delineated by palpation. The mucous membrane of the trachea was minimally incised along the right-hand border of the tumor and a mucosal flap was elevated. The left side of the trachea including the membranous wall and cartilage of the tracheal mucosa was maximally preserved, to maintain the vascular supply to the trachea. Finally, the membranous wall of the trachea was preserved to within one-third of the left-hand side. Furthermore, the risk of bleeding from major lateral vessels was reduced. A sternocleidomastoid muscle flap was elevated and inserted into the cavity resulting from the tumor resection and sutured between the esophagus and trachea. The membranous wall of the tracheal mucosa was also sutured submucosally.
Results: The tumor was removed completely with the muscular layer of the esophagus without injury to the intact recurrent laryngeal nerve and lateral major vessels. The patient started oral nutritional intake on the first postoperative day and was discharged without any significant postoperative complications.
Conclusions: This new procedure for transtracheal resection for recurrent thyroid cancer involving the trachea and esophagus was useful and safe.
Figures
References
-
- Patel KN, Shaha AR. Poorly differentiated and anaplastic thyroid cancer. Cancer Control. 2006;13:119–128. - PubMed
-
- Volante M, Collini P, Nikiforov YE, Sakamoto A, Kakudo K, Katoh R, Lloyd RV, LiVolsi VA, Papotti M, Sobrinho-Simoes M, Bussolati G, Rosai J. Poorly differentiated thyroid carcinoma: the Turin proposal for the use of uniform diagnostic criteria and an algorithmic diagnostic approach. Am J Surg Pathol. 2007;31:1256–1264. doi: 10.1097/PAS.0b013e3180309e6a. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
