

Understanding reasons for treatment interruption amongst patients on antiretroviral therapy--a qualitative study at the Lighthouse Clinic, Lilongwe, Malawi
- PMID: 25280736
- PMCID: PMC4185090
- DOI: 10.3402/gha.v7.24795
Understanding reasons for treatment interruption amongst patients on antiretroviral therapy--a qualitative study at the Lighthouse Clinic, Lilongwe, Malawi
Abstract
Background: In recent years, scaling up of antiretroviral therapy (ART) in resource-limited settings moved impressively towards universal access. Along with these achievements, public health HIV programs are facing a number of challenges including the support of patients on lifelong therapy and the prevention of temporary/permanent loss of patients in care. Understanding reasons for treatment interruption (TI) can inform strategies for improving drug adherence and retention in care.
Objective: To evaluate key characteristics of patients resuming ART after TI at the Lighthouse Clinic in Lilongwe, Malawi, and to identify their reasons for interrupting ART.
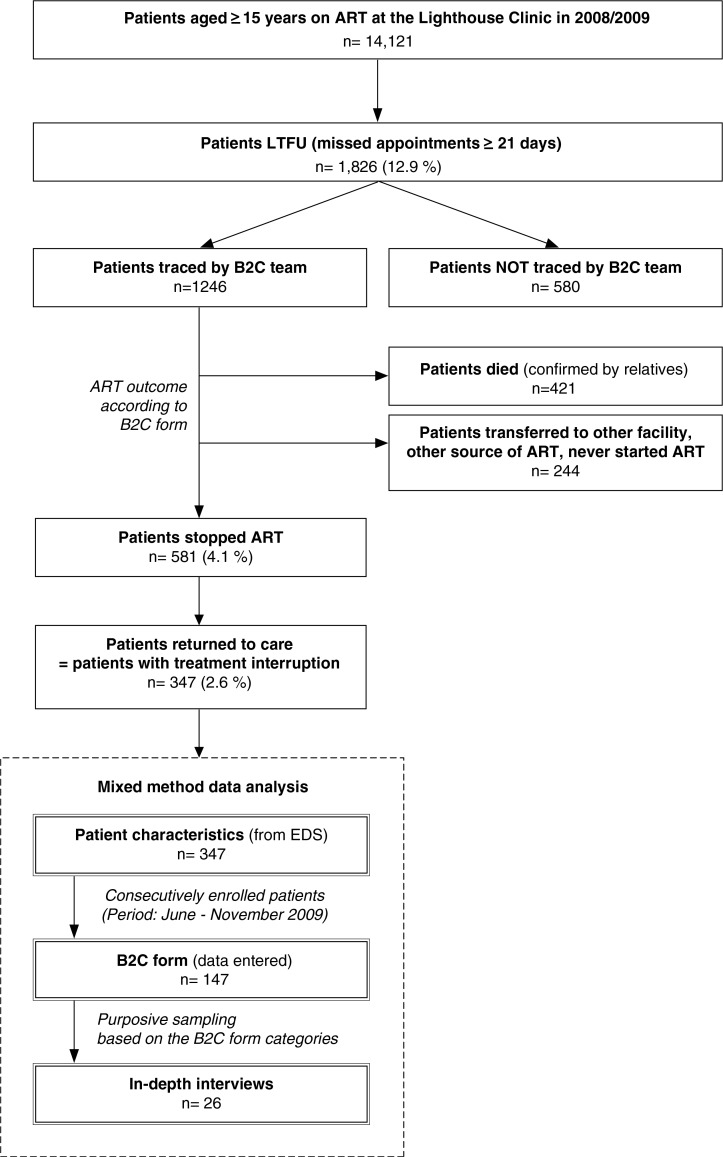
Design: This study uses a mixed methods design to evaluate patients resuming ART after TI. We analysed an assessment form for patients with TI using pre-defined categories and a comments field to identify frequently stated reasons for TI. Additionally, we conducted 26 in-depth interviews to deepen our understanding of common reasons for TI. In-depth interviews also included the patients' knowledge about ART and presence of social support systems. Qualitative data analysis was based on a thematic framework approach.
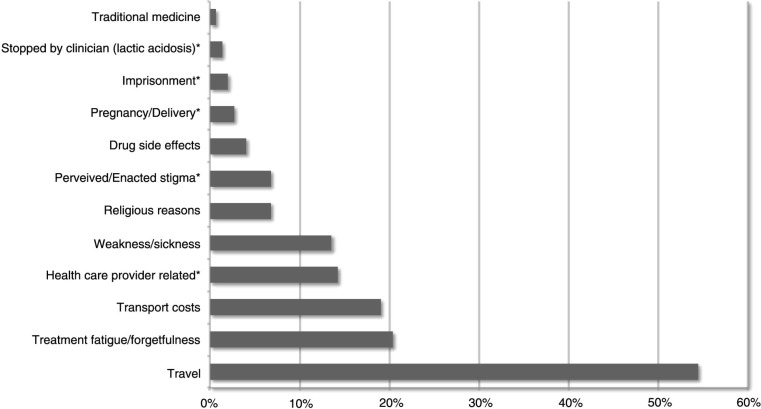
Results: A total of 347 patients (58.2% female, average age 35.1±11.3 years) with TI were identified. Despite the presence of social support and sufficient knowledge of possible consequences of TI, all patients experienced situations that resulted in TI. Analysis of in-depth interviews led to new and distinct categories for TI. The most common reason for TI was travel (54.5%, n=80/147), which further differentiated into work- or family-related travel. Patients also stated transport costs and health-care-provider-related reasons, which included perceived/enacted discrimination by health care workers. Other drivers of TI were treatment fatigue/forgetfulness, the patients' health status, adverse drug effects, pregnancy/delivery, religious belief or perceived/enacted stigma.
Conclusions: To adequately address patients' needs on a lifelong therapy, adherence-counselling sessions require provision of problem-solving strategies for common barriers to continuous care.
Keywords: Malawi; adherence; antiretroviral therapy; retention in care; treatment interruption.
Figures
Similar articles
-
Factors influencing adherence to antiretroviral treatment among adults accessing care from private health facilities in Malawi.BMC Public Health. 2019 Oct 28;19(1):1382. doi: 10.1186/s12889-019-7768-z. BMC Public Health. 2019. PMID: 31660947 Free PMC article.
-
Barriers and facilitators to patients' adherence to antiretroviral treatment in Zambia: a qualitative study.SAHARA J. 2008 Sep;5(3):136-43. doi: 10.1080/17290376.2008.9724912. SAHARA J. 2008. PMID: 18979047
-
Barriers to HIV Treatment Adherence: A Qualitative Study of Discrepancies Between Perceptions of Patients and Health Providers in Tanzania and Uganda.AIDS Patient Care STDS. 2019 Sep;33(9):406-413. doi: 10.1089/apc.2019.0053. AIDS Patient Care STDS. 2019. PMID: 31517526 Free PMC article.
-
Mapping patient-identified barriers and facilitators to retention in HIV care and antiretroviral therapy adherence to Andersen's Behavioral Model.AIDS Care. 2015;27(7):817-28. doi: 10.1080/09540121.2015.1009362. Epub 2015 Feb 11. AIDS Care. 2015. PMID: 25671515 Free PMC article. Review.
-
Exploring 'generative mechanisms' of the antiretroviral adherence club intervention using the realist approach: a scoping review of research-based antiretroviral treatment adherence theories.BMC Public Health. 2017 May 4;17(1):385. doi: 10.1186/s12889-017-4322-8. BMC Public Health. 2017. PMID: 28472938 Free PMC article.
Cited by
-
How much does it cost to retain antiretroviral therapy (ART) clients in care? Routine financial costs of retention interventions at Lighthouse Trust's Martin Preuss Centre (MPC) in Lilongwe, Malawi.Res Sq [Preprint]. 2023 Dec 22:rs.3.rs-3773952. doi: 10.21203/rs.3.rs-3773952/v1. Res Sq. 2023. Update in: BMC Res Notes. 2025 Mar 07;18(1):101. doi: 10.1186/s13104-024-07077-z. PMID: 38196659 Free PMC article. Updated. Preprint.
-
A qualitative approach to understand antiretroviral therapy (ART) adherence for refugees living in Nakivale Refugee Settlement in Uganda.Confl Health. 2018 Mar 12;12:7. doi: 10.1186/s13031-018-0145-1. eCollection 2018. Confl Health. 2018. PMID: 29545828 Free PMC article.
-
Individual, household, and community level barriers to ART adherence among women in rural Eswatini.PLoS One. 2020 Apr 28;15(4):e0231952. doi: 10.1371/journal.pone.0231952. eCollection 2020. PLoS One. 2020. PMID: 32343742 Free PMC article.
-
How HIV Clients Find Their Way Back to the ART Clinic: A Qualitative Study of Disengagement and Re-engagement with HIV Care in Malawi.AIDS Behav. 2022 Mar;26(3):674-685. doi: 10.1007/s10461-021-03427-1. Epub 2021 Aug 17. AIDS Behav. 2022. PMID: 34403022 Free PMC article.
-
How much does it cost to retain clients on antiretroviral treatment for one year in a large, public clinic? Routine financial costs of retention interventions at Lighthouse Trust in Lilongwe, Malawi.BMC Res Notes. 2025 Mar 7;18(1):101. doi: 10.1186/s13104-024-07077-z. BMC Res Notes. 2025. PMID: 40055806 Free PMC article.
References
-
- Schwartlander B, Grubb I, Perriens J. The 10-year struggle to provide antiretroviral treatment to people with HIV in the developing world. Lancet. 2006;368:541–6. - PubMed
-
- UNAIDS. Global report: UNAIDS report on the global AIDS epidemic 2012. unaids.org. 2012. Available from: http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiolo... [cited 19 April 2013].
-
- Egger M, May M, Chêne G, Phillips AN, Ledergerber B, Dabis F, et al. Prognosis of HIV-1-infected patients starting highly active antiretroviral therapy: a collaborative analysis of prospective studies. Lancet. 2002;360:119–29. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical