

Cardiac remodeling in response to 1 year of intensive endurance training
- PMID: 25281664
- PMCID: PMC5698012
- DOI: 10.1161/CIRCULATIONAHA.114.010775
Cardiac remodeling in response to 1 year of intensive endurance training
Abstract
Background: It is unclear whether, and to what extent, the striking cardiac morphological manifestations of endurance athletes are a result of exercise training or a genetically determined characteristic of talented athletes. We hypothesized that prolonged and intensive endurance training in previously sedentary healthy young individuals could induce cardiac remodeling similar to that observed cross-sectionally in elite endurance athletes.
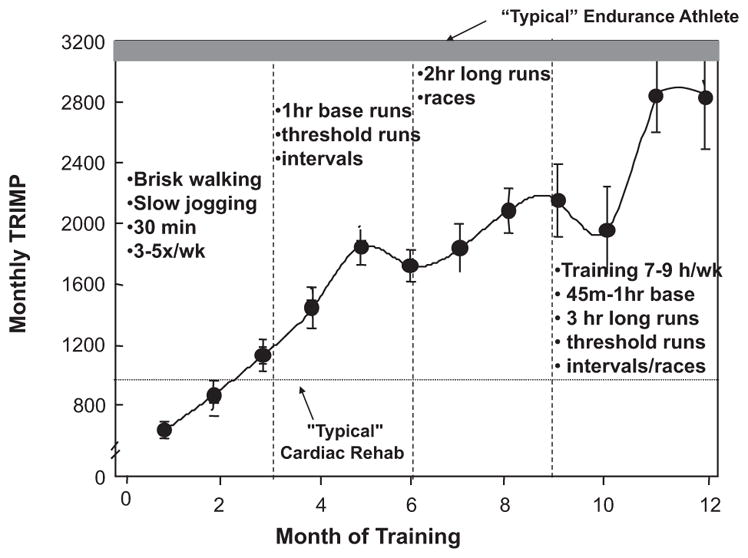
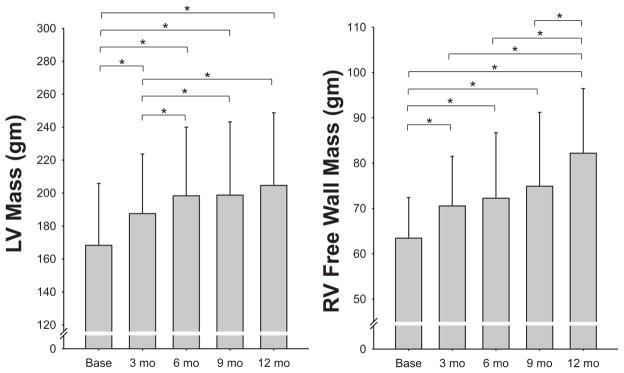
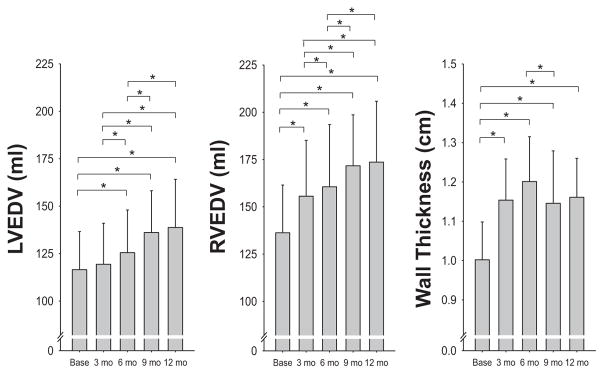
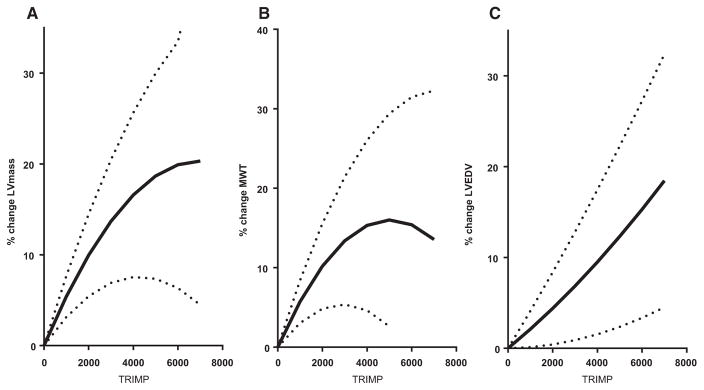
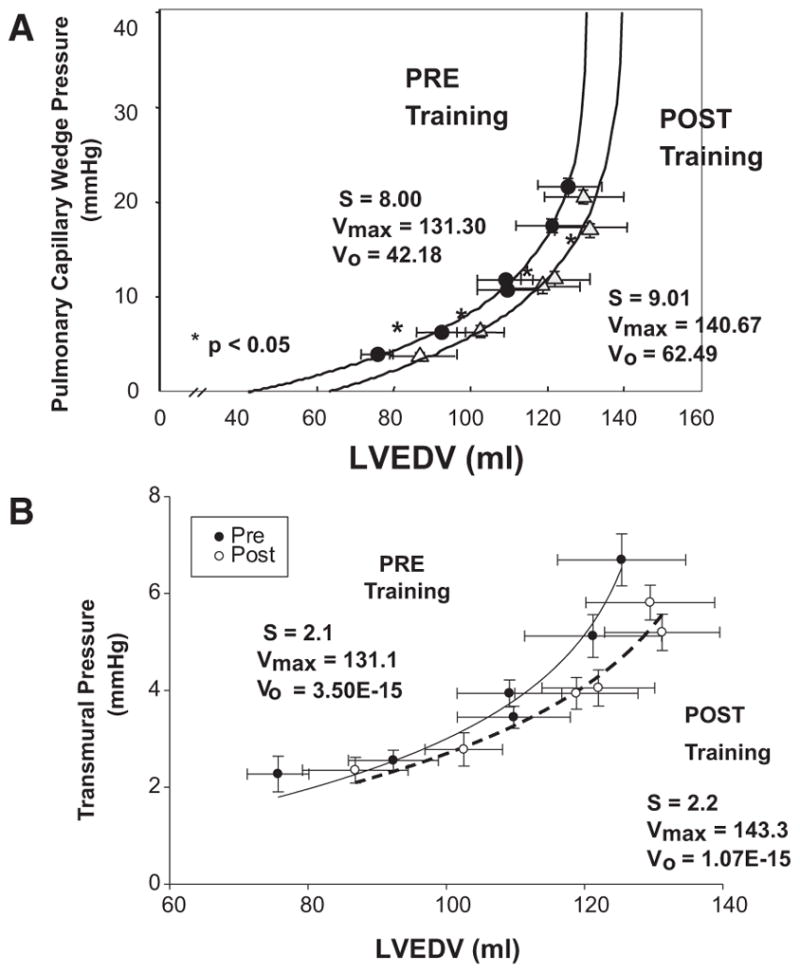
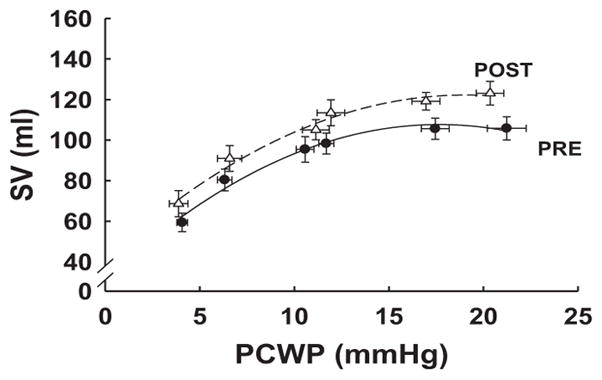
Methods and results: Twelve previously sedentary subjects (aged 29±6 years; 7 men and 5 women) trained progressively and intensively for 12 months such that they could compete in a marathon. Magnetic resonance images for assessment of right and left ventricular mass and volumes were obtained at baseline and after 3, 6, 9, and 12 months of training. Maximum oxygen uptake ( max) and cardiac output at rest and during exercise (C2H2 rebreathing) were measured at the same time periods. Pulmonary artery catheterization was performed before and after 1 year of training, and pressure-volume and Starling curves were constructed during decreases (lower body negative pressure) and increases (saline infusion) in cardiac volume. Mean max rose from 40.3±1.6 to 48.7±2.5 mL/kg per minute after 1 year (P<0.00001), associated with an increase in both maximal cardiac output and stroke volume. Left and right ventricular mass increased progressively with training duration and intensity and reached levels similar to those observed in elite endurance athletes. In contrast, left ventricular volume did not change significantly until 6 months of training, although right ventricular volume increased progressively from the outset; Starling and pressure-volume curves approached but did not match those of elite athletes.
Conclusions: One year of prolonged and intensive endurance training leads to cardiac morphological adaptations in previously sedentary young subjects similar to those observed in elite endurance athletes; however, it is not sufficient to achieve similar levels of cardiac compliance and performance. Contrary to conventional thinking, the left ventricle responds to exercise with initial concentric but not eccentric remodeling during the first 6 to 9 months after commencement of endurance training depending on the duration and intensity of exercise. Thereafter, the left ventricle dilates and restores the baseline mass-to-volume ratio. In contrast, the right ventricle responds to endurance training with eccentric remodeling at all levels of training.
Keywords: exercise; exercise nutrition physiology; hypertrophy.
© 2014 American Heart Association, Inc.
Figures
Comment in
-
Letter by Sanchis-Gomar et al Regarding Article, "Cardiac Remodeling in Response to 1 Year of Intensive Endurance Training".Circulation. 2015 Sep 15;132(11):e146. doi: 10.1161/CIRCULATIONAHA.114.013764. Circulation. 2015. PMID: 26371240 No abstract available.
References
-
- Levine BD, Buckey JC, Fritsch JM, Yancy CW, Jr, Watenpaugh DE, Snell PG, Lane LD, Eckberg DL, Blomqvist CG. Physical fitness and cardiovascular regulation: mechanisms of orthostatic intolerance. J Appl Physiol (1985) 1991;70:112–122. - PubMed
-
- Di Bello V, Santoro G, Talarico L, Di Muro C, Caputo MT, Giorgi D, Bertini A, Bianchi M, Giusti C. Left ventricular function during exercise in athletes and in sedentary men. Med Sci Sports Exerc. 1996;28:190–196. - PubMed
-
- Stickland MK, Welsh RC, Petersen SR, Tyberg JV, Anderson WD, Jones RL, Taylor DA, Bouffard M, Haykowsky MJ. Does fitness level modulate the cardiovascular hemodynamic response to exercise? J Appl Physiol (1985) 2006;100:1895–1901. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
