

Deciphering the complexities of atopic dermatitis: shifting paradigms in treatment approaches
- PMID: 25282559
- PMCID: PMC4186710
- DOI: 10.1016/j.jaci.2014.08.008
Deciphering the complexities of atopic dermatitis: shifting paradigms in treatment approaches
Abstract
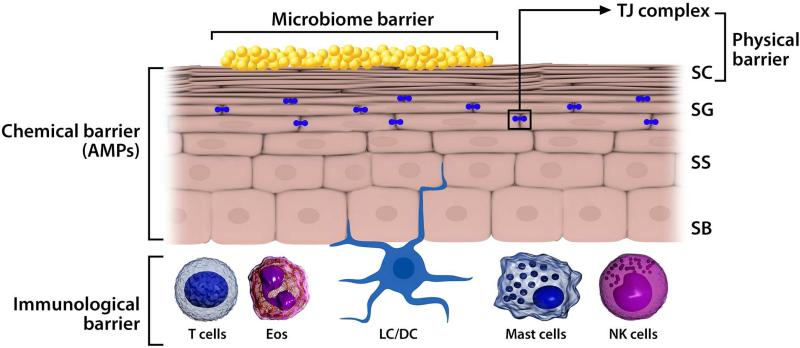
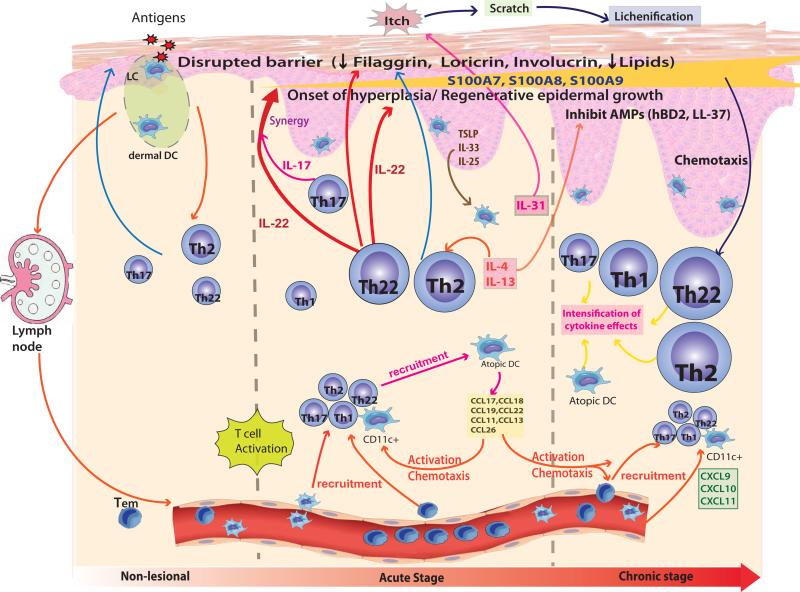
Atopic dermatitis (AD) is the most common chronic inflammatory skin disease. It often precedes the development of food allergy and asthma. Recent insights into AD reveal abnormalities in terminal differentiation of the epidermal epithelium leading to a defective stratum corneum, which allows enhanced allergen penetration and systemic IgE sensitization. Atopic skin is also predisposed to colonization or infection by pathogenic microbes, most notably Staphylococcus aureus and herpes simplex virus. Causes of this abnormal skin barrier are complex and driven by a combination of genetic, environmental, and immunologic factors. These factors likely account for the heterogeneity of AD onset and the severity and natural history of this skin disease. Recent studies suggest prevention of AD can be achieved through early interventions to protect the skin barrier. Onset of lesional AD requires effective control of local and systemic immune activation for optimal management. Early intervention might improve long-term outcomes for AD and reduce the systemic allergen sensitization that leads to associated allergic diseases in the gastrointestinal and respiratory tract.
Keywords: Atopic dermatitis; eczema; filaggrin; immune; infection; skin epithelium.
Copyright © 2014 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Figures


References
-
- Schmitt J, Langan S, Deckert S, Svensson A, von Kobyletzki L, Thomas K, et al. Assessment of clinical signs of atopic dermatitis: a systematic review and recommendation. J Allergy Clin Immunol. 2013;132:1337–47. - PubMed
-
- McLean WH, Palmer CN, Henderson J, Kabesch M, Weidinger S, Irvine AD. Filaggrin variants confer susceptibility to asthma. J Allergy Clin Immunol. 2008;121:1294–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
