

Comparison of hybrid procedure and open surgical revascularization for multilevel infrainguinal arterial occlusive disease
- PMID: 25284992
- PMCID: PMC4181442
- DOI: 10.2147/CIA.S66860
Comparison of hybrid procedure and open surgical revascularization for multilevel infrainguinal arterial occlusive disease
Abstract
Objective: To compare outcomes of hybrid (combined surgical and endovascular) procedures (HYBRID) with open surgical reconstructions (OPEN) in patients with multilevel infrainguinal artery occlusive diseases.
Design: Case series study with retrospective analysis of prospectively collected nonrandomized data.
Methods: Between 2008 and 2012, 64 patients underwent OPEN and 43 underwent HYBRID. Patient characteristics, technique success, clinical improvement, and procedure-related morbidity were reviewed and compared. Patency rates and limb salvages were analyzed and compared using Kaplan-Meier life tables. Cox regression analyses were used to assess the influence of various risk factors on primary patency.
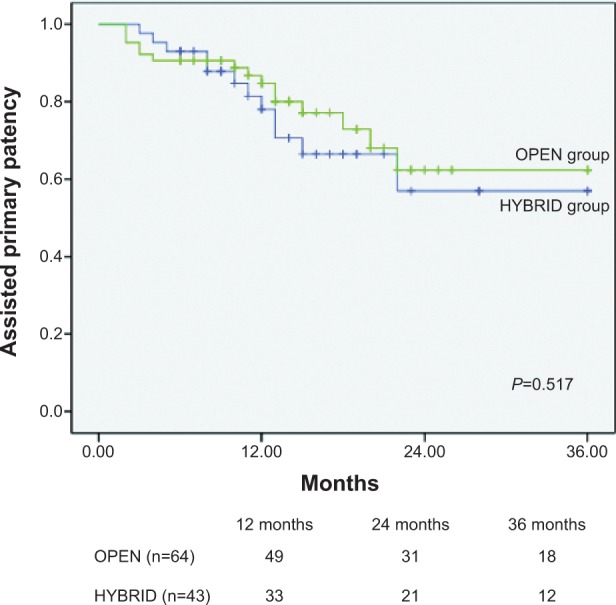
Results: HYBRID patients were older and presented with worse New York Heart Association function compared with OPEN patients. The increase in the ankle-brachial index and improvement of Ruthford category after procedures were equivalent between two groups, but HYBRID patients had shorter hospital length of stay (7.6±12.0 versus 15.5±17.3; P= 0.018) and less overall perioperative morbidity (12% versus 28%; P=0.042) compared with OPEN patients. No statistically significant difference in 36-month primary (47.1%±7.1% versus 50.1%±9.4%; P=0.418), assisted primary (57.0%±7.9% versus 62.4%±9.2%; P=0.517), or secondary (82.0%±6.8% versus 83.1%±7.3%; P=0.445) patency was seen between the two groups. Limb salvage rates of HYBRID vs OPEN at 3 years were similar (76.3%±9.3% versus 80.4%±8.2%; P=0.579). Critical limb ischemia was a negative predictor of long-term patency of patients in both the HYBRID and OPEN groups (P=0.012 and P<0.001, respectively), and the presence of diabetes and renal insufficiency were another two independent predictors of decreased primary patency for HYBRID (P=0.017 and P=0.019, respectively).
Conclusion: Multilevel infrainguinal artery occlusive diseases could be treated by hybrid procedure, with shorter hospitalization, less perioperative morbidity, and similar early- and long-term efficacy compared with open revascularization. A hybrid procedure should be considered for patients with high surgical risk, but critical limb ischemia, diabetes, and renal insufficiency could compromise its long-term patency.
Keywords: atherosclerotic occlusive disease; endovascular treatment; hybrid procedure.
Figures



Similar articles
-
[The use of hybrid revascularization procedures for the therapy of multilevel lower extremity arterial disease--analysis of single center experience].Rozhl Chir. 2015 Sep;94(9):372-8. Rozhl Chir. 2015. PMID: 26537102 Czech.
-
Iliac artery stenting combined with open femoral endarterectomy is as effective as open surgical reconstruction for severe iliac and common femoral occlusive disease.J Vasc Surg. 2011 Aug;54(2):402-11. doi: 10.1016/j.jvs.2011.01.027. Epub 2011 Apr 30. J Vasc Surg. 2011. PMID: 21531527
-
Combined percutaneous endovascular iliac angioplasty and infrainguinal surgical revascularization for chronic lower extremity ischemia: preliminary result.Vascular. 2010 Mar-Apr;18(2):71-6. doi: 10.2310/6670.2010.00007. Vascular. 2010. PMID: 20338130
-
Meta-analysis of direct surgical versus endovascular revascularization for aortoiliac occlusive disease.J Vasc Surg. 2020 Aug;72(2):726-737. doi: 10.1016/j.jvs.2019.12.035. Epub 2020 Mar 11. J Vasc Surg. 2020. PMID: 32171442
-
Hybrid procedures for peripheral obstructive disease.J Cardiovasc Surg (Torino). 2010 Dec;51(6):833-43. J Cardiovasc Surg (Torino). 2010. PMID: 21124279 Review.
Cited by
-
A Decade of Progress: Assessing Three Revascularization Strategies for Iliac Occlusive Disease Through a 580-Case, 10-Year-Experience Literature Comparison.Cureus. 2024 Aug 13;16(8):e66826. doi: 10.7759/cureus.66826. eCollection 2024 Aug. Cureus. 2024. PMID: 39280387 Free PMC article.
-
Lower extremity revascularization via endovascular and surgical approaches: A systematic review with emphasis on combined inflow and outflow revascularization.SAGE Open Med. 2020 Jun 4;8:2050312120929239. doi: 10.1177/2050312120929239. eCollection 2020. SAGE Open Med. 2020. PMID: 32551113 Free PMC article. Review.
-
Femorofemoral artery bypass grafting in aortoiliac occlusive disease patients: A case report.Int J Surg Case Rep. 2022 Oct;99:107689. doi: 10.1016/j.ijscr.2022.107689. Epub 2022 Sep 19. Int J Surg Case Rep. 2022. PMID: 36150331 Free PMC article.
-
Comparison and Trends of Endovascular, Surgical and Hybrid Revascularizations and the Influence of Comorbidity in 1 Million Hospitalizations Due to Peripheral Artery Disease in Germany Between 2009 and 2018.Cardiovasc Intervent Radiol. 2022 Oct;45(10):1472-1482. doi: 10.1007/s00270-022-03136-9. Epub 2022 Apr 15. Cardiovasc Intervent Radiol. 2022. PMID: 35428938 Free PMC article.
References
-
- Lyden SP, Smouse HB. TASC II and the endovascular management of infrainguinal disease. J Endovasc Ther. 2009;16(2(suppl 2)):II5–II18. - PubMed
-
- Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, TASC II Working Group Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II) J Vasc Surg. 2007;45(Suppl S):S5–S67. - PubMed
-
- Van Den Berg J, Waser S, Trelle S, Diehm N, Baumgartner I. Lesion characteristics of patients with chronic critical limb ischemia that determine choice of treatment modality. J Cardiovasc Surg (Torino) 2012;53(1):45–52. - PubMed
-
- Dougherty MJ, Young LP, Calligaro KD. One hundred twenty-five concomitant endovascular and open procedures for lower extremity arterial disease. J Vasc Surg. 2003;37(2):316–322. - PubMed
-
- Balaz P, Rokosny S, Bafrnec J, Björck M. The role of hybrid procedures in the management of peripheral vascular disease. Scand J Surg. 2012;101(4):232–237. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
