

Further insight into the cardiovascular risk calculator: the roles of statins, revascularizations, and underascertainment in the Women's Health Study
- PMID: 25285455
- PMCID: PMC4394380
- DOI: 10.1001/jamainternmed.2014.5336
Further insight into the cardiovascular risk calculator: the roles of statins, revascularizations, and underascertainment in the Women's Health Study
Abstract
Importance: While the pooled cohort equations from the recent American College of Cardiology/American Heart Association (ACC/AHA) Guideline on the Assessment of Cardiovascular Risk have overestimated cardiovascular risk in multiple external cohorts, the reasons for the discrepancy are unclear.
Objective: To determine whether increased use of statins over time, incident coronary revascularization procedures, or underascertainment of vascular events explain overestimation of risk in a more contemporary population.
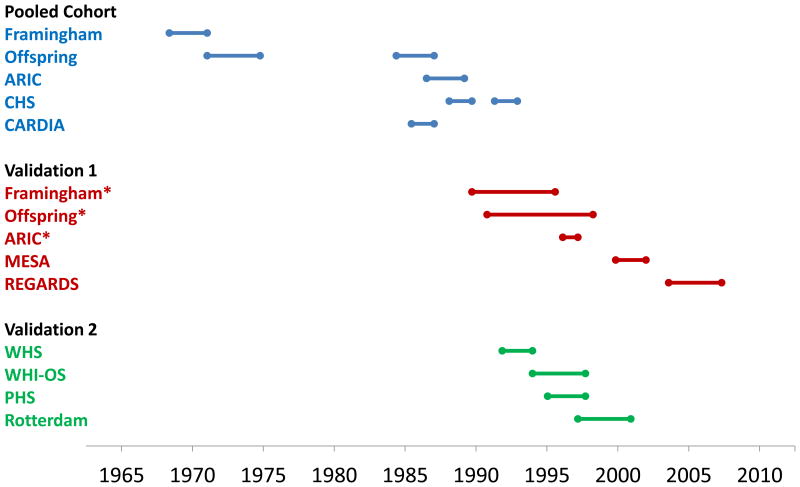
Design, setting, and participants: The Women's Health Study (WHS) is a nationwide cohort of US women free of cardiovascular disease, cancer, or other major illness at baseline from 1992 to 1995. A total of 27 542 women ages 45 to 79 years with complete ascertainment of plasma lipids and other risk factors were followed for a median of 10 years.
Main outcome and measure: Atherosclerotic cardiovascular disease (ASCVD), defined as any myocardial infarction, any stroke, or death due to cardiovascular cause.
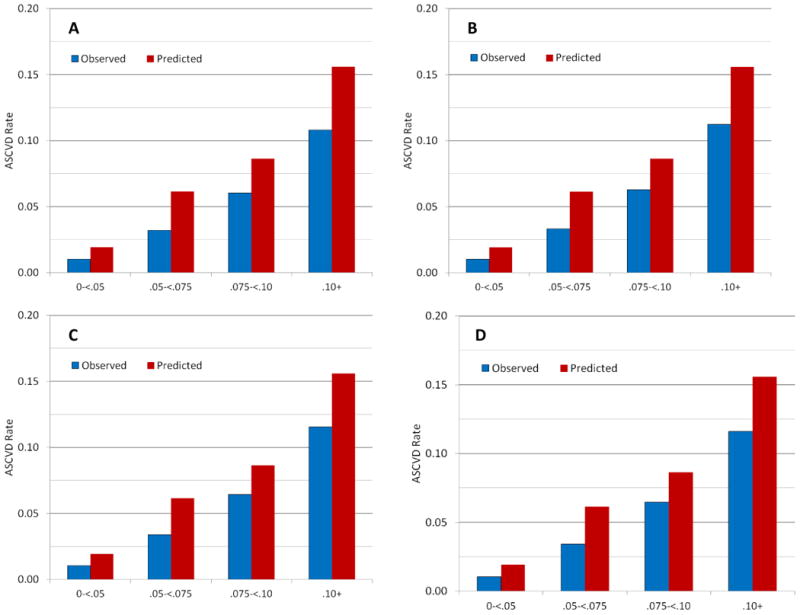
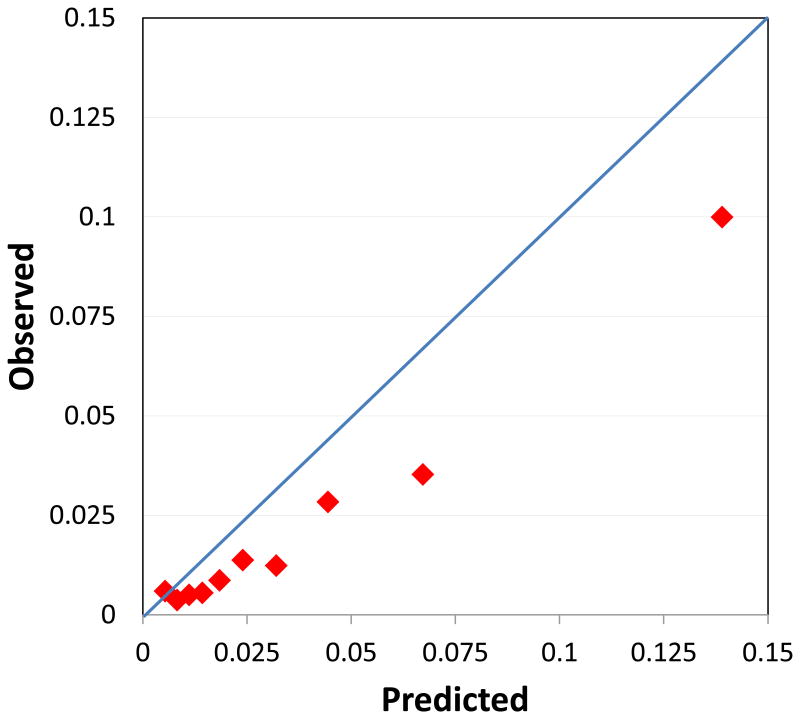
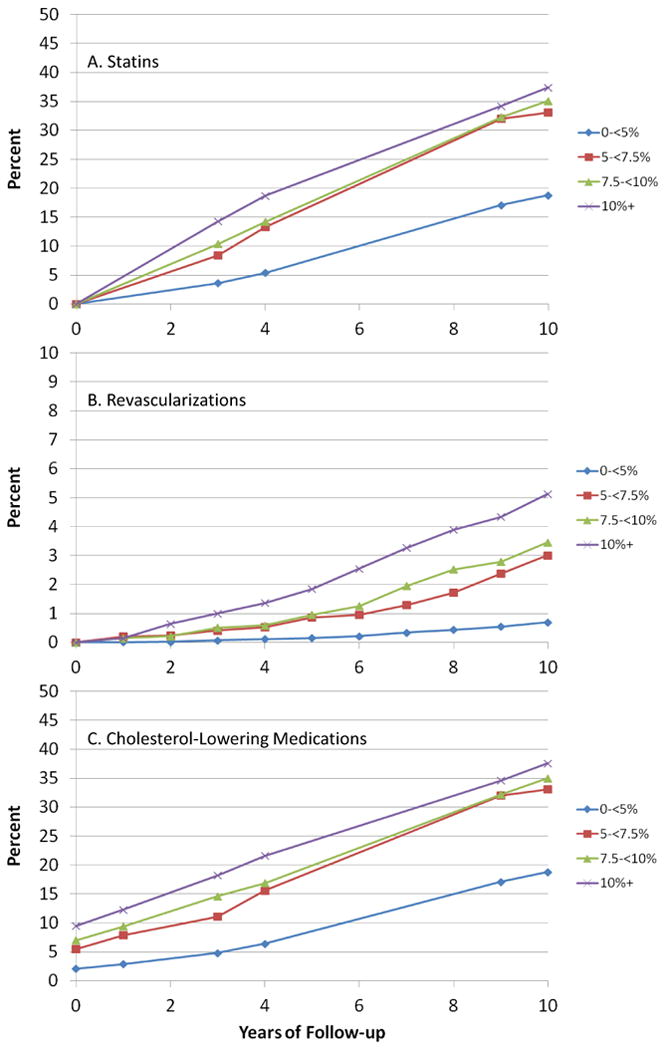
Results: A total of 632 women experienced an ASCVD event over the course of the follow-up. The average predicted risk from the pooled cohort equations was 3.6% over 10 years, compared with an actual observed risk of 2.2%. Ratios of predicted to observed rates were 1.90 or higher in the groups with 0 to less than 5.0% and 5.0% to less than 7.5% risk and were over 1.40 in the groups with 7.5% to less than 10.0% and 10.0% or higher risk. Rates of statin use and revascularizations increased over follow-up time and by risk group, and in sensitivity analyses, we estimated the hypothetical rates if no women were prescribed statins or underwent revascularization procedures. After adjustment for intervention effects of statins and revascularization as well as hypothetical confounding by indication, ratios of predicted to observed rates remained 1.80 or higher in the lower 2 risk groups and over 1.30 higher in the upper 2 risk groups. Underascertainment is unlikely since follow-up rates in the WHS were 97.2%, and overall we would need approximately 60% more events to match the numbers predicted using the pooled cohort equations.
Conclusions and relevance: Statin use, revascularization procedures, and underascertainment of events do not explain the discrepancy between observed rates of ASCVD in the WHS and those predicted by the ACC/AHA pooled cohort equations. Other explanations include changing patterns of risk within more contemporary populations.
Figures
Comment in
-
Prevention guidelines: bad process, bad outcome.JAMA Intern Med. 2014 Dec;174(12):1972-3. doi: 10.1001/jamainternmed.2014.3278. JAMA Intern Med. 2014. PMID: 25285604 No abstract available.
-
Further insight into the cardiovascular risk calculator: time to rethink the strategy?JAMA Intern Med. 2015 May;175(5):862. doi: 10.1001/jamainternmed.2015.69. JAMA Intern Med. 2015. PMID: 25938311 No abstract available.
References
-
- Goff DC, Jr, Lloyd-Jones DM, Bennett G, et al. 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(suppl 2):S49–S73. - PubMed
-
- Ridker PM, Cook NR. Statins: new American guidelines for prevention of cardiovascular disease. Lancet. 2013;382:1762–1765. - PubMed
-
- Kavousi M, Leening MJG, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, Adult Treatment Panel III guidelines, and European Society of Cardiology guidelines for cardiovascular disease prevention in a European cohort. JAMA. 2014;311(14):1416–1423. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
