

Efficacy and tolerability of 3 nonnucleoside reverse transcriptase inhibitor-sparing antiretroviral regimens for treatment-naive volunteers infected with HIV-1: a randomized, controlled equivalence trial
- PMID: 25285539
- PMCID: PMC4412467
- DOI: 10.7326/M14-1084
Efficacy and tolerability of 3 nonnucleoside reverse transcriptase inhibitor-sparing antiretroviral regimens for treatment-naive volunteers infected with HIV-1: a randomized, controlled equivalence trial
Erratum in
- Ann Intern Med. 2014 Nov 4;161(9):680
Abstract
Background: Nonnucleoside reverse transcriptase inhibitor-based antiretroviral therapy is not suitable for all treatment-naive HIV-infected persons.
Objective: To evaluate 3 nonnucleoside reverse transcriptase inhibitor-sparing initial antiretroviral regimens to show equivalence for virologic efficacy and tolerability.
Design: A phase 3, open-label study randomized in a 1:1:1 ratio with follow-up for at least 96 weeks. (ClinicalTrials.gov: NCT00811954).
Setting: 57 sites in the United States and Puerto Rico.
Patients: Treatment-naive persons aged 18 years or older with HIV-1 RNA levels greater than 1000 copies/mL without resistance to nucleoside reverse transcriptase inhibitors or protease inhibitors.
Intervention: Atazanavir, 300 mg/d, with ritonavir, 100 mg/d; raltegravir, 400 mg twice daily; or darunavir, 800 mg/d, with ritonavir, 100 mg/d, plus combination emtricitabine, 200 mg/d, and tenofovir disoproxil fumarate, 300 mg/d.
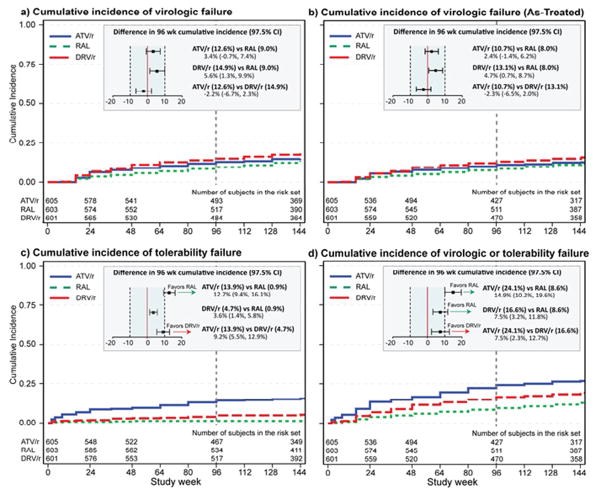
Measurements: Virologic failure, defined as a confirmed HIV-1 RNA level greater than 1000 copies/mL at or after 16 weeks and before 24 weeks or greater than 200 copies/mL at or after 24 weeks, and tolerability failure, defined as discontinuation of atazanavir, raltegravir, or darunavir for toxicity. A secondary end point was a combination of virologic efficacy and tolerability.
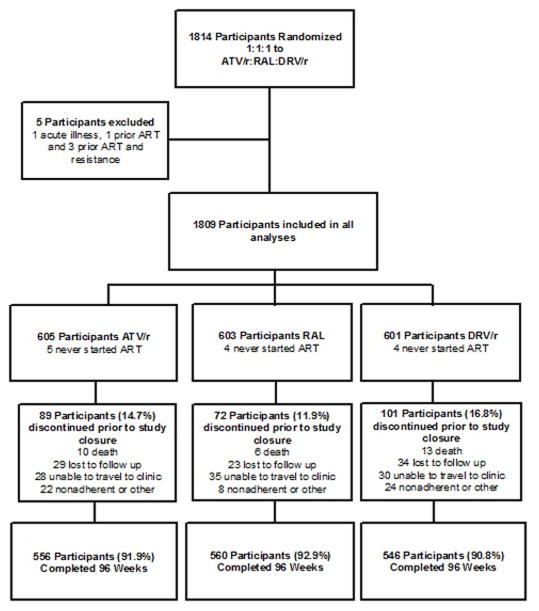
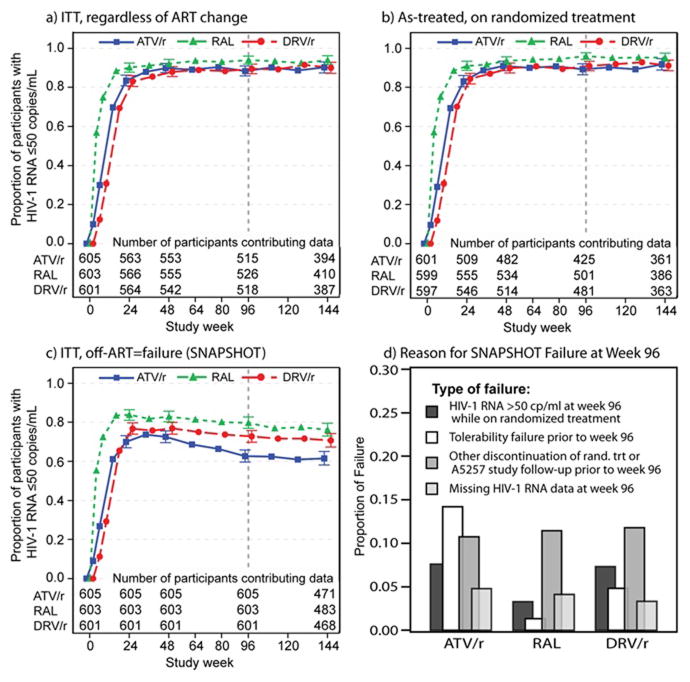
Results: Among 1809 participants, all pairwise comparisons of incidence of virologic failure over 96 weeks showed equivalence within a margin of equivalence defined as -10% to 10%. Raltegravir and ritonavir-boosted darunavir were equivalent for tolerability, whereas ritonavir-boosted atazanavir resulted in a 12.7% and 9.2% higher incidence of tolerability discontinuation than raltegravir and ritonavir-boosted darunavir, respectively, primarily because of hyperbilirubinemia. For combined virologic efficacy and tolerability, ritonavir-boosted darunavir was superior to ritonavir-boosted atazanavir, and raltegravir was superior to both protease inhibitors. Antiretroviral resistance at the time of virologic failure was rare but more frequent with raltegravir.
Limitation: The trial was open-label, and ritonavir was not provided.
Conclusion: Over 2 years, all 3 regimens attained high and equivalent rates of virologic control. Tolerability of regimens containing raltegravir or ritonavir-boosted darunavir was superior to that of the ritonavir-boosted atazanavir regimen.
Primary funding source: National Institute of Allergy and Infectious Diseases.
Comment in
-
Three nonnucleoside reverse transcriptase inhibitor-sparing antiretroviral regimens for treatment-naive volunteers infected with HIV-1.Ann Intern Med. 2015 Mar 17;162(6):460-1. doi: 10.7326/L15-5066. Ann Intern Med. 2015. PMID: 25775332 No abstract available.
-
Three nonnucleoside reverse transcriptase inhibitor-sparing antiretroviral regimens for treatment-naive volunteers infected with HIV-1.Ann Intern Med. 2015 Mar 17;162(6):461. doi: 10.7326/L15-5066-2. Ann Intern Med. 2015. PMID: 25775333 No abstract available.
-
Three nonnucleoside reverse transcriptase inhibitor-sparing antiretroviral regimens for treatment-naive volunteers infected with HIV-1.Ann Intern Med. 2015 Mar 17;162(6):461-2. doi: 10.7326/L15-5066-3. Ann Intern Med. 2015. PMID: 25775334 No abstract available.
Summary for patients in
-
Summaries for patients. Nonnucleoside reverse transcriptase inhibitor-sparing antiretroviral regimens for treatment-naive volunteers infected with HIV-1.Ann Intern Med. 2014 Oct 7;161(7):I-22. doi: 10.7326/P14-9035. Ann Intern Med. 2014. PMID: 25285557 No abstract available.
References
-
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services; [Accessed 3 June 2014]. Available at http://aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf.
-
- World Health Organization. WHO Conslolidated Guildeines on the use of Antiretroviral Drugs for Treating and Preventing HIV Infection: recommendations for a public health approach. Geneva, Switzerland: 2013. pp. 1–272. - PubMed
-
- Periard D, Telenti A, Sudre P, Cheseaux JJ, Halfon P, Reymond MJ, et al. Atherogenic dyslipidemia in HIV-infected individuals treated with protease inhibitors. The Swiss HIV Cohort Study. Circulation. 1999;100(7):700–5. - PubMed
-
- Worm SW, Kamara DA, Reiss P, Fontas E, De Wit S, El-Sadr W, et al. Evaluation of HIV protease inhibitor use and the risk of sudden death or nonhemorrhagic stroke. J Infect Dis. 2012;205(4):535–9. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- 2 UM1 AI068636-08/AI/NIAID NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- UL1 RR024160/RR/NCRR NIH HHS/United States
- P30 AI060354/AI/NIAID NIH HHS/United States
- UM1AI68634/AI/NIAID NIH HHS/United States
- UM1 AI069494/AI/NIAID NIH HHS/United States
- UM1 AI069423/AI/NIAID NIH HHS/United States
- UM1 AI069503/AI/NIAID NIH HHS/United States
- 2UM1AI069503-08/AI/NIAID NIH HHS/United States
- 2UM1AI069439-08/AI/NIAID NIH HHS/United States
- U01 TR000445/TR/NCATS NIH HHS/United States
- 2UM1 AI069418-08/AI/NIAID NIH HHS/United States
- UL1 TR000445/TR/NCATS NIH HHS/United States
- UM1AI069439/AI/NIAID NIH HHS/United States
- AI069556/AI/NIAID NIH HHS/United States
- U01 AI069447/AI/NIAID NIH HHS/United States
- UM1 AI069501/AI/NIAID NIH HHS/United States
- UM1 AI069472/AI/NIAID NIH HHS/United States
- P30 AI050409/AI/NIAID NIH HHS/United States
- UL1 TR001111/TR/NCATS NIH HHS/United States
- U01AI069447/AI/NIAID NIH HHS/United States
- UL1TR000124/TR/NCATS NIH HHS/United States
- 1U01AI069494/AI/NIAID NIH HHS/United States
- UM1 AI069424/AI/NIAID NIH HHS/United States
- 2UM1-AI069470-08/AI/NIAID NIH HHS/United States
- 5UM1 AI069484-07/AI/NIAID NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- 2UM1AI069432/AI/NIAID NIH HHS/United States
- 2UM1AI069452-08/AI/NIAID NIH HHS/United States
- UM1 AI069432/AI/NIAID NIH HHS/United States
- AI069501/AI/NIAID NIH HHS/United States
- AI-069471/AI/NIAID NIH HHS/United States
- AI 69501/AI/NIAID NIH HHS/United States
- 2UM1AI069412-08/AI/NIAID NIH HHS/United States
- UM1-AI069534-08/AI/NIAID NIH HHS/United States
- UM1 AI069471/AI/NIAID NIH HHS/United States
- U01 AI069439/AI/NIAID NIH HHS/United States
- U01 AI069556/AI/NIAID NIH HHS/United States
- U01 AI069418/AI/NIAID NIH HHS/United States
- UM1 AI069494./AI/NIAID NIH HHS/United States
- UM1 AI069534/AI/NIAID NIH HHS/United States
- UL1 RR024156/RR/NCRR NIH HHS/United States
- UM1 AI069439/AI/NIAID NIH HHS/United States
- UM1AI069494/AI/NIAID NIH HHS/United States
- UL1TR000058/TR/NCATS NIH HHS/United States
- UL1 TR000124/TR/NCATS NIH HHS/United States
- P30 AI50410/AI/NIAID NIH HHS/United States
- UM1 AI069415/AI/NIAID NIH HHS/United States
- 5U01 AI069471/AI/NIAID NIH HHS/United States
- UL1 TR024160/TR/NCATS NIH HHS/United States
- UM1AI069419/AI/NIAID NIH HHS/United States
- UL1 TR000058/TR/NCATS NIH HHS/United States
- AI069439/AI/NIAID NIH HHS/United States
- P30 AI045008/AI/NIAID NIH HHS/United States
- UM1 AI069484/AI/NIAID NIH HHS/United States
- UM1 AI068634/AI/NIAID NIH HHS/United States
- U01 AI069501/AI/NIAID NIH HHS/United States
- UM1 AI069412/AI/NIAID NIH HHS/United States
- UM1 AI069470/AI/NIAID NIH HHS/United States
- 1UL1TR001111/TR/NCATS NIH HHS/United States
- UM1 AI069481/AI/NIAID NIH HHS/United States
- 2UM1 AI069511-08/AI/NIAID NIH HHS/United States
- UM AI069481/AI/NIAID NIH HHS/United States
- UM1 AI069477/AI/NIAID NIH HHS/United States
- U01 AI069432/AI/NIAID NIH HHS/United States
- P30 AI028697/AI/NIAID NIH HHS/United States
- UL1TR000457/TR/NCATS NIH HHS/United States
- UM1 AI069423-08/AI/NIAID NIH HHS/United States
- U01 AI068636/AI/NIAID NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- UM1 AI069452/AI/NIAID NIH HHS/United States
- UM1 AI069496/AI/NIAID NIH HHS/United States
- AI069424/AI/NIAID NIH HHS/United States
- 5UL1 RR024156;/RR/NCRR NIH HHS/United States
- 2UM1AI069415-09/AI/NIAID NIH HHS/United States
- UM1 AI069556/AI/NIAID NIH HHS/United States
- P30 AI027763/AI/NIAID NIH HHS/United States
- UL1TR000439/TR/NCATS NIH HHS/United States
- UL1TR001079/TR/NCATS NIH HHS/United States
- UL1 TR000170/TR/NCATS NIH HHS/United States
- UL1 TR001082/TR/NCATS NIH HHS/United States
- UM1 AI106701/AI/NIAID NIH HHS/United States
- UM1 AI069532/AI/NIAID NIH HHS/United States
- UM1 AI069465/AI/NIAID NIH HHS/United States
- U01 AI069424/AI/NIAID NIH HHS/United States
- 2UM1 AI069465/AI/NIAID NIH HHS/United States
- 5-P30-AI-045008-15/AI/NIAID NIH HHS/United States
- UM1 AI069419/AI/NIAID NIH HHS/United States
- UL1 RR025008/RR/NCRR NIH HHS/United States
- AI069432/AI/NIAID NIH HHS/United States
- UL1 TR000004/TR/NCATS NIH HHS/United States
- U01 AI069477/AI/NIAID NIH HHS/United States
- UM1AI069472/AI/NIAID NIH HHS/United States
- UL1 TR000457/TR/NCATS NIH HHS/United States
- UM1 AI069511/AI/NIAID NIH HHS/United States
- U01 AI069494/AI/NIAID NIH HHS/United States
- AI69432/AI/NIAID NIH HHS/United States
- 2 UM1 AI069503-08/AI/NIAID NIH HHS/United States
- UM1AI068636/AI/NIAID NIH HHS/United States
- AI069477/AI/NIAID NIH HHS/United States
- AI069471/AI/NIAID NIH HHS/United States
- U01 AI069471/AI/NIAID NIH HHS/United States
- UM1 AI068636/AI/NIAID NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- UM1 AI069418/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases