

NGF blockade at early times during bone cancer development attenuates bone destruction and increases limb use
- PMID: 25287160
- PMCID: PMC4253026
- DOI: 10.1158/0008-5472.CAN-14-1220
NGF blockade at early times during bone cancer development attenuates bone destruction and increases limb use
Abstract
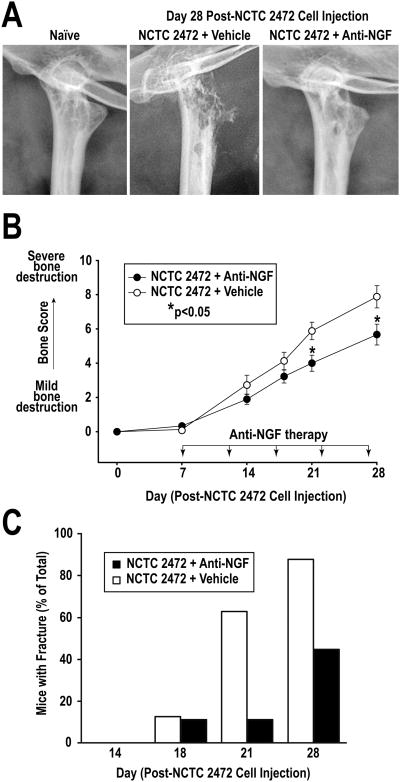
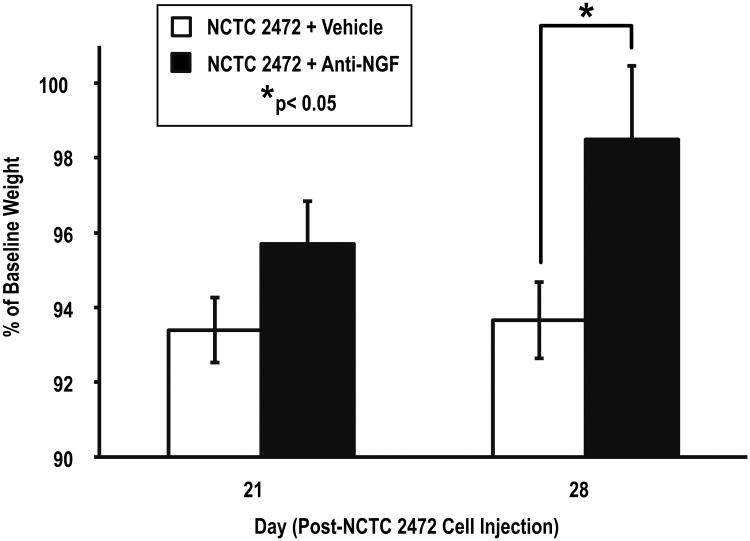
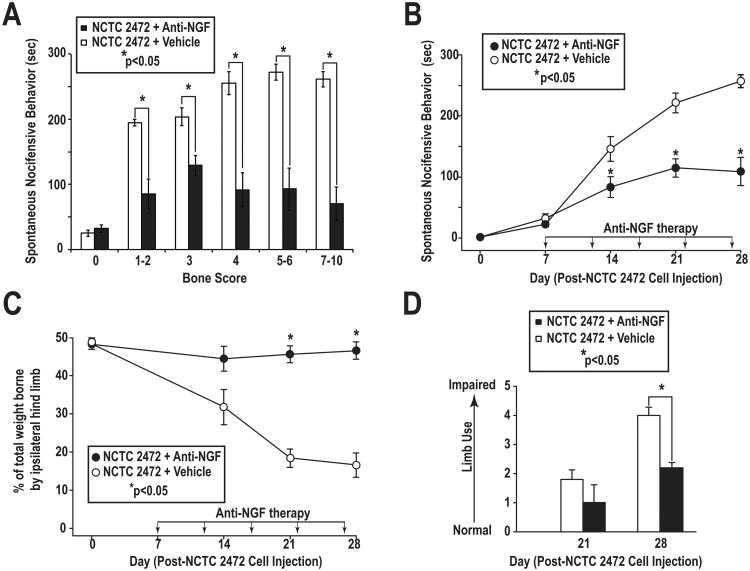
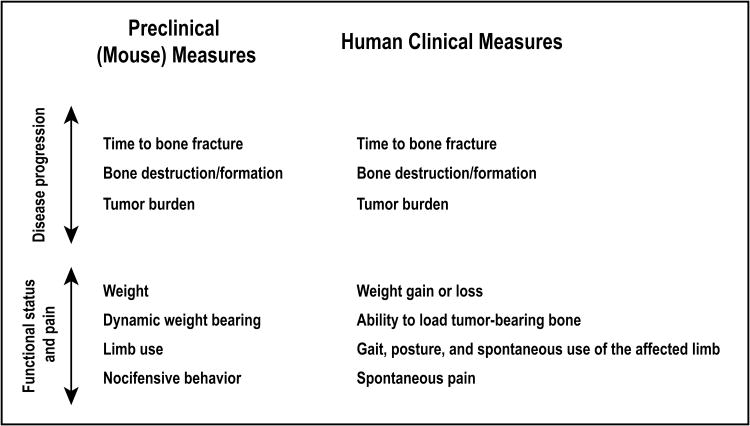
Studies in animals and humans show that blockade of nerve growth factor (NGF) attenuates both malignant and nonmalignant skeletal pain. While reduction of pain is important, a largely unanswered question is what other benefits NGF blockade might confer in patients with bone cancer. Using a mouse graft model of bone sarcoma, we demonstrate that early treatment with an NGF antibody reduced tumor-induced bone destruction, delayed time to bone fracture, and increased the use of the tumor-bearing limb. Consistent with animal studies in osteoarthritis and head and neck cancer, early blockade of NGF reduced weight loss in mice with bone sarcoma. In terms of the extent and time course of pain relief, NGF blockade also reduced pain 40% to 70%, depending on the metric assessed. Importantly, this analgesic effect was maintained even in animals with late-stage disease. Our results suggest that NGF blockade immediately upon detection of tumor metastasis to bone may help preserve the integrity and use, delay the time to tumor-induced bone fracture, and maintain body weight.
©2014 American Association for Cancer Research.
Conflict of interest statement
Figures

References
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. - PubMed
-
- Ibrahim T, Farolfi A, Mercatali L, Ricci M, Amadori D. Metastatic bone disease in the era of bone-targeted therapy: clinical impact. Tumori. 2013;99:1–9. - PubMed
-
- Cancer.org. American Cancer Society, Inc.; 2014. [updated 2013 Dec 31; cited 2013 Apr 5]. Internet. Available from: http://www.cancer.org/research/cancerfactsstatistics/cancerfactsfigures2....
-
- Farrell C. Bone metastases: assessment, management and treatment options. Br J Nurs. 2013;22:S4, S6, S8–11. - PubMed
-
- von Moos R, Sternberg C, Body JJ, Bokemeyer C. Reducing the burden of bone metastases: current concepts and treatment options. Support Care Cancer. 2013;21:1773–83. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
