

Final safety and efficacy of erlotinib in the phase 4 POLARSTAR surveillance study of 10 708 Japanese patients with non-small-cell lung cancer
- PMID: 25287435
- PMCID: PMC4317960
- DOI: 10.1111/cas.12550
Final safety and efficacy of erlotinib in the phase 4 POLARSTAR surveillance study of 10 708 Japanese patients with non-small-cell lung cancer
Abstract
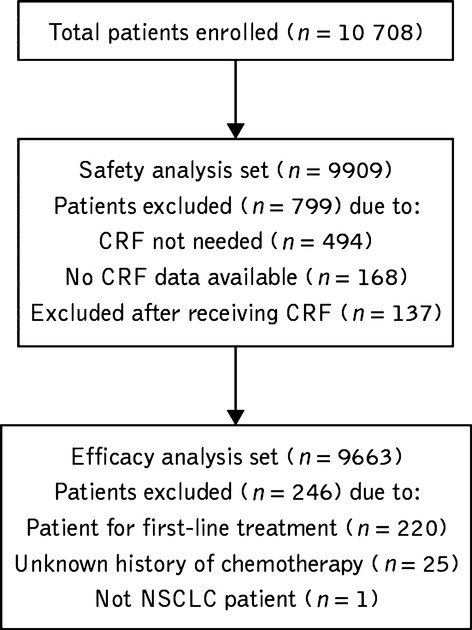
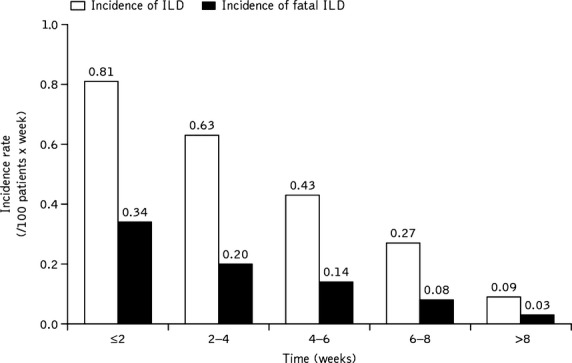
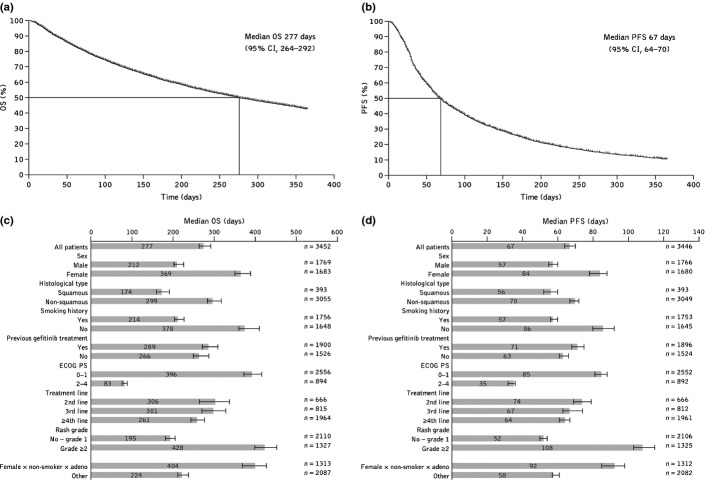
Interstitial lung disease (ILD) occurrence and risk factors were investigated in the Japanese non-small-cell lung cancer, post-marketing, large-scale surveillance study, POLARSTAR. All patients with unresectable, recurrent/advanced non-small-cell lung cancer who were treated with erlotinib in Japan between December 2007 and October 2009 were enrolled. Primary endpoints were patterns of ILD and risk factors for onset of ILD and ILD-related death. Overall survival, progression-free survival, and occurrence of adverse drug reactions were secondary endpoints. Interstitial lung disease was confirmed in 429 (4.3%) patients. Concurrent/previous ILD (hazard ratio, 3.19), emphysema or chronic obstructive pulmonary disease (hazard ratio, 1.86), lung infection (hazard ratio, 1.55), smoking history (hazard ratio, 2.23), and period from initial cancer diagnosis to the start of treatment (<360 days; hazard ratio, 0.58) were identified as significant risk factors for developing ILD by Cox multivariate analysis. Logistic regression analysis identified Eastern Cooperative Oncology Group performance status 2-4 (odds ratio, 2.45 [95% confidence interval, 1.41-4.27]; P = 0.0016), ≤50% remaining normal lung area (odds ratio, 3.12 [1.48-6.58]; P = 0.0029), and concomitant honeycombing with interstitial pneumonia (odds ratio, 6.67 [1.35-32.94]; P = 0.02) as poor prognostic factors for ILD death. Median overall survival was 277 days; median progression-free survival was 67 days. These data confirm the well-characterized safety profile of erlotinib. Interstitial lung disease is still an adverse drug reaction of interest in this population, and these results, including ILD risk factors, give helpful information for treatment selection and monitoring. Erlotinib efficacy was additionally confirmed in this population. (POLARSTAR trial ML21590.).
Keywords: Erlotinib; Japanese; interstitial lung disease; non-small-cell lung cancer; surveillance.
© 2014 The Authors. Cancer Science published by Wiley Publishing Asia Pty Ltd on behalf of Japanese Cancer Association.
Figures
References
-
- Shepherd F, Pereira J, Ciuleanu T, et al. Erlotinib in previously treated non-small-cell lung cancer. New Engl J Med. 2005;353:123–32. - PubMed
-
- Kubota K, Nishiwaki Y, Tamura T, et al. Efficacy and safety of erlotinib monotherapy for Japanese patients with advanced non-small cell lung cancer: a phase II study. J Thorac Oncol. 2008;3:1439–45. - PubMed
-
- Takahashi T, Yamamoto N, Nukiwa T, et al. Phase II study of erlotinib in Japanese patients with advanced non-small cell lung cancer. Anticancer Res. 2010;30:557–63. - PubMed
-
- Yamamoto N, Horiike A, Fujisaka Y, et al. Phase I dose-finding and pharmacokinetic study of the oral epidermal growth factor receptor tyrosine kinase inhibitor Ro50–8231 (erlotinib) in Japanese patients with solid tumors. Cancer Chemother Pharmacol. 2008;61:489–96. - PubMed
-
- Yoshida S. The results of gefitinib prospective investigation. Med Drug J. 2005;41:772–89.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
