

Preventing ARDS: progress, promise, and pitfalls
- PMID: 25288000
- PMCID: PMC4188145
- DOI: 10.1378/chest.14-0555
Preventing ARDS: progress, promise, and pitfalls
Abstract
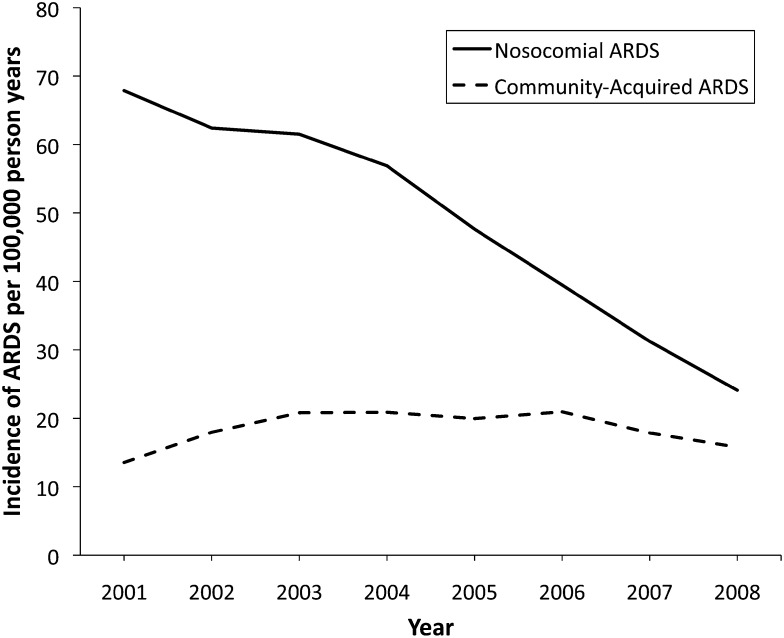
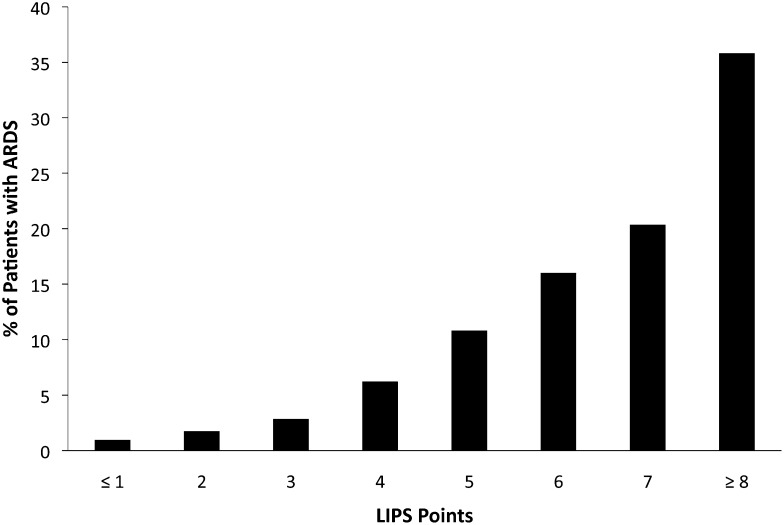
Advances in critical care practice have led to a substantial decline in the incidence of ARDS over the past several years. Low tidal volume ventilation, timely resuscitation and antimicrobial administration, restrictive transfusion practices, and primary prevention of aspiration and nosocomial pneumonia have likely contributed to this reduction. Despite decades of research, there is no proven pharmacologic treatment of ARDS, and mortality from ARDS remains high. Consequently, recent initiatives have broadened the scope of lung injury research to include targeted prevention of ARDS. Prediction scores have been developed to identify patients at risk for ARDS, and clinical trials testing aspirin and inhaled budesonide/formoterol for ARDS prevention are ongoing. Future trials aimed at preventing ARDS face several key challenges. ARDS has not been validated as an end point for pivotal clinical trials, and caution is needed when testing toxic therapies that may prevent ARDS yet potentially increase mortality.
Figures
References
-
- Ciesla DJ, Moore EE, Johnson JL, et al. Decreased progression of postinjury lung dysfunction to the acute respiratory distress syndrome and multiple organ failure. Surgery. 2006;140(4):640-647 - PubMed
-
- The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301-1308 - PubMed
-
- Serpa Neto A, Cardoso SO, Manetta JA, et al. Association between use of lung-protective ventilation with lower tidal volumes and clinical outcomes among patients without acute respiratory distress syndrome: a meta-analysis. JAMA. 2012;308(16):1651-1659 - PubMed
-
- Futier E, Constantin JM, Paugam-Burtz C, et al. ; IMPROVE Study Group. A trial of intraoperative low-tidal-volume ventilation in abdominal surgery. N Engl J Med. 2013;369(5):428-437 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
