

Propensity-based study of aminoglycoside nephrotoxicity in patients with severe sepsis or septic shock
- PMID: 25288085
- PMCID: PMC4249539
- DOI: 10.1128/AAC.03750-14
Propensity-based study of aminoglycoside nephrotoxicity in patients with severe sepsis or septic shock
Abstract
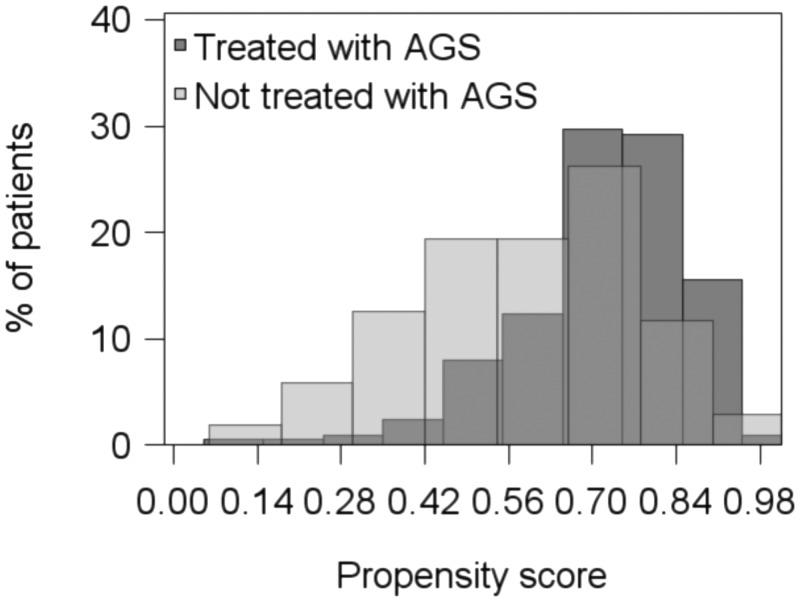
To assess the risk of acute kidney injury (AKI) attributable to aminoglycosides (AGs) in patients with severe sepsis or septic shock, we performed a retrospective cohort study in one medical intensive care unit (ICU) in France. Patients admitted for severe sepsis/septic shock between November 2008 and January 2010 were eligible. A propensity score for AG administration was built using day 1 demographic and clinical characteristics. Patients still on the ICU on day 3 were included. Patients with renal failure before day 3 or endocarditis were excluded. The time window for assessment of renal risk was day 3 to day 15, defined according to the RIFLE (risk, injury, failure, loss, and end-stage renal disease) classification. The AKI risk was assessed by means of a propensity-adjusted Cox proportional hazards regression analysis. Of 317 consecutive patients, 198 received AGs. The SAPS II (simplified acute physiology score II) score and nosocomial origin of infection favored the use of AGs, whereas a preexisting renal insufficiency and the neurological site of infection decreased the propensity for AG treatment. One hundred three patients with renal failure before day 3 were excluded. AGs were given once daily over 2.6 ± 1.1 days. AKI occurred in 16.3% of patients in a median time of 6 (interquartile range, 5 to 10) days. After adjustment to the clinical course and exposure to other nephrotoxic agents between day 1 and day 3, a propensity-adjusted Cox proportional hazards regression analysis showed no increased risk of AKI in patients receiving AGs (adjusted relative risk = 0.75 [0.32 to 1.76]). In conclusion, in critically septic patients presenting without early renal failure, aminoglycoside therapy for less than 3 days was not associated with an increased risk of AKI.
Copyright © 2014, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Paul M, Benuri-Silbiger I, Soares-Weiser K, Leibovici L. 2004. Beta lactam monotherapy versus beta lactam-aminoglycoside combination therapy for sepsis in immunocompetent patients: systematic review and meta-analysis of randomised trials. BMJ 328:668. 10.1136/bmj.38028.520995.63. - DOI - PMC - PubMed
-
- Kumar A, Safdar N, Kethireddy S, Chateau D. 2010. A survival benefit of combination antibiotic therapy for serious infections associated with sepsis and septic shock is contingent only on the risk of death: a meta-analytic/meta-regression study. Crit. Care Med. 38:1651–1664. 10.1097/CCM.0b013e3181e96b91. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
