

Diagnostic yield and morbidity by neuronavigation-guided frameless stereotactic biopsy using magnetic resonance imaging and by frame-based computed tomography-guided stereotactic biopsy
- PMID: 25289174
- PMCID: PMC4173323
- DOI: 10.4103/2152-7806.140211
Diagnostic yield and morbidity by neuronavigation-guided frameless stereotactic biopsy using magnetic resonance imaging and by frame-based computed tomography-guided stereotactic biopsy
Abstract
Background: We compared the diagnostic yield and morbidity by frame-based computed tomography-guided stereotactic biopsy (CTSTB) with Brown-Roberts-Wells (BRW) unit and by neuronavigation-guided frameless stereotactic biopsy (NSTB) using magnetic resonance imaging (MRI).
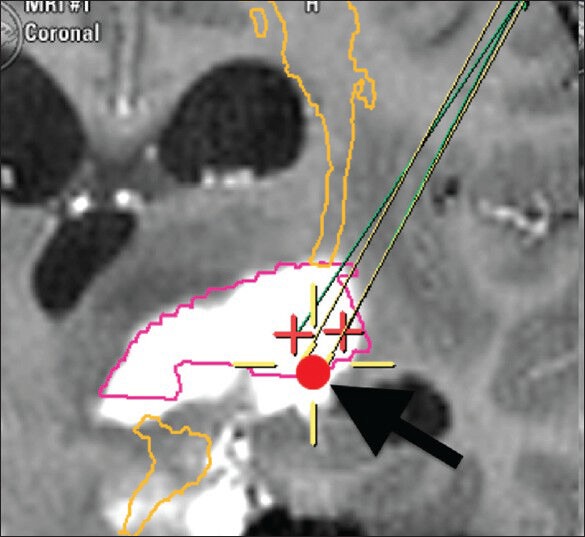
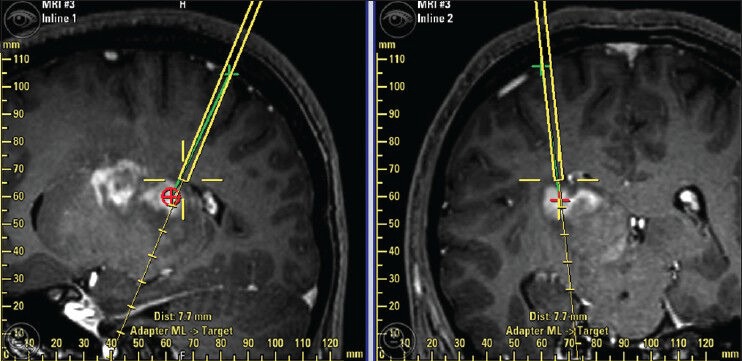
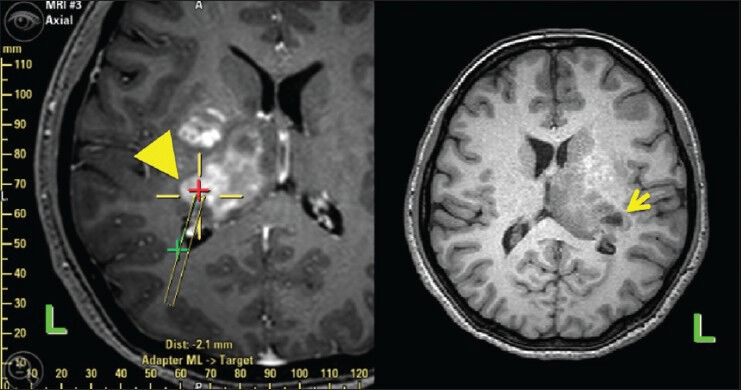
Methods: The subjects' age range was 15-83 years. CTSTB with BRW unit was performed for 59 tumors (58 cases, 1988-2007). NSTB was performed for 38 tumors (35 cases, 2007-2013) with the needle sheath attached to the head holder. By NSTB, target locations of sampling points and trajectories were confirmed by using MRI. Diffusion tensor imaging-based fiber tractography was used to achieve safe trajectories. STB by using BRW did not visualize the trajectory virtually; however, the planning images for NSTB were able to show the trajectory virtually before the procedure.
Results: Histological diagnoses were established for 93 tumors at the first biopsy. The diagnostic yield was 94.9% by CTSTB and 97.4% by NSTB (P = 0.944). The morbidity rate was 5.1% by CTSTB and 0% by NSTB (P = 0.417). The absolute risk reduction was 23.1% by NSTB when the targets were basal ganglia (putamen, globus pallidus) or thalamus. In the cases of glioma for which the targets were basal ganglia (putamen, globus pallidus) or thalamus, the absolute risk reduction by NSTB was 30%.
Conclusions: There was no significant difference between CTSTB and NSTB concerning the diagnostic yield and morbidity. However, when the target is the basal ganglia (putamen, globus pallidus) or thalamus and glioma is suspected, NSTB by using MRI with virtual trajectory is preferable to CTSTB concerning morbidity.
Keywords: Brain tumor; neuronavigation; stereotactic biopsy.
Figures
References
-
- Apuzzo ML, Chandrasoma PT, Cohen D, Zee CS, Zelman V. Computed imaging stereotaxy: Experience and perspective related to 500 procedures applied to brain masses. Neurosurgery. 1987;20:930–7. - PubMed
-
- Apuzzo ML, Sabshin JK. Computed tomographic guidance stereotaxis in the management of intracranial mass lesions. Neurosurgery. 1983;12:277–85. - PubMed
-
- Dammers R, Haitsma IK, Schouten JW, Kros JM, Avezaat CJ, Vincent AJ. Safety and efficacy of frameless and frame-based intracranial biopsy techniques. Acta Neurochir (Wien) 2008;150:23–9. - PubMed
-
- Dorward NL, Paleologos TS, Alberti O, Thomas DG. The advantages of frameless stereotactic biopsy over frame-based biopsy. Br J Neurosurg. 2002;16:110–8. - PubMed
-
- Gralla J, Nimsky C, Buchfelder M, Fahlbusch R, Ganslandt O. Frameless stereotactic brain biopsy procedures using the Stealth Station: Indications, accuracy and results. Zentralbl Neurochir. 2003;64:166–70. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
