

Prospective clinical study of 551 cases of liposuction and abdominoplasty performed individually and in combination
- PMID: 25289226
- PMCID: PMC4174197
- DOI: 10.1097/GOX.0b013e3182a333d7
Prospective clinical study of 551 cases of liposuction and abdominoplasty performed individually and in combination
Abstract
Background: Despite the popularity of these procedures, there are limited published prospective studies evaluating liposuction and abdominoplasty. Lipoabdominoplasty is a subject of recent attention. Several investigators have recommended alternative techniques that preserve the Scarpa fascia in an effort to reduce complications, particularly the risk of seromas.
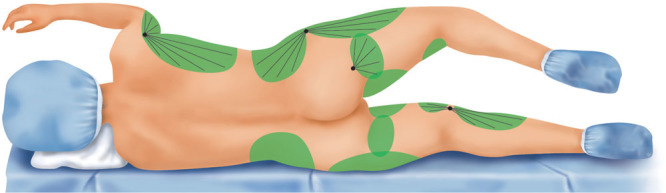
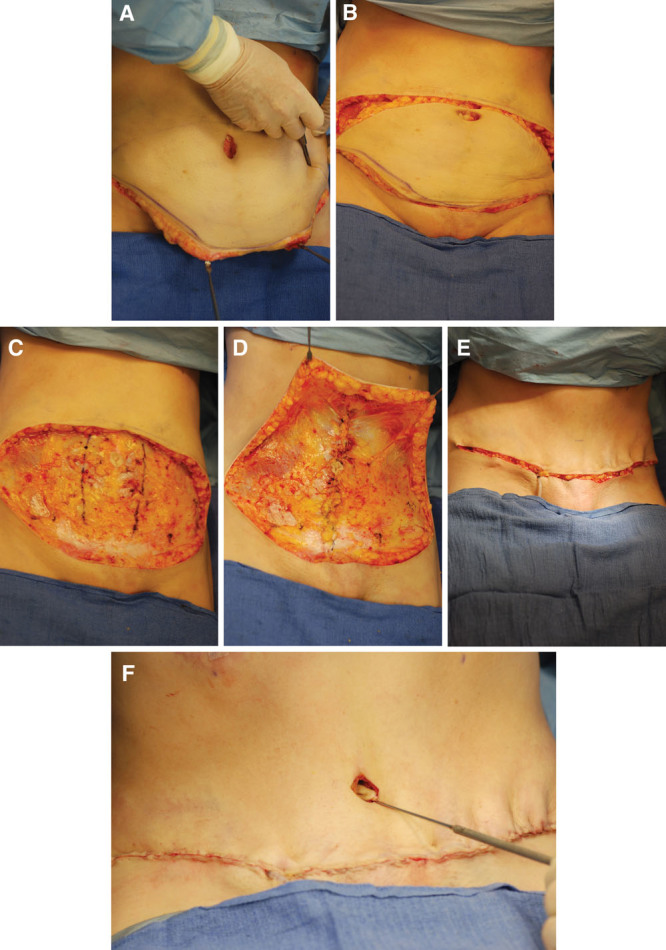
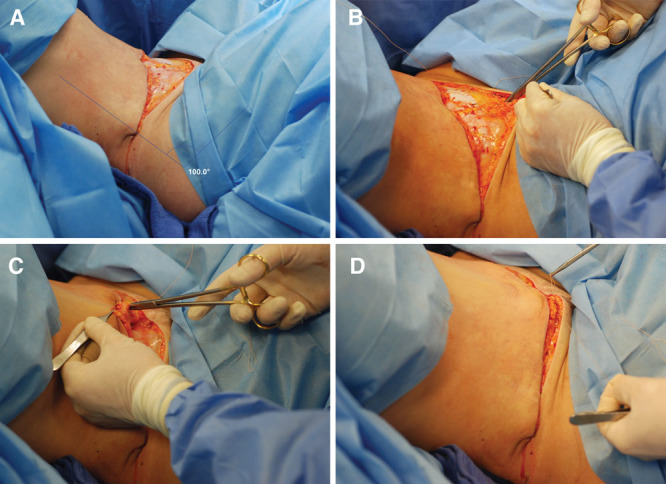
Methods: Over a 5-year period, 551 consecutive patients were treated with ultrasonic liposuction alone (n = 384), liposuction/abdominoplasty (n = 150), or abdominoplasty alone (n = 17). In lipoabdominoplasties, the abdomen and flanks were first treated with liposuction. A traditional flap dissection was used for all abdominoplasties. Scalpel dissection was used rather than electrodissection. A supine "jackknife" position was used in surgery to provide maximum hip flexion, allowing a secure deep fascial repair.
Results: The complication rate after liposuction was 4.2% vs 50% for patients treated with an abdominoplasty. Approximately half of the abdominoplasty complications were minor scar deformities, including widened umbilical scars (17.3%) that were revised. The seroma rate after abdominoplasties was 5.4%; there were no seromas after liposuction alone.
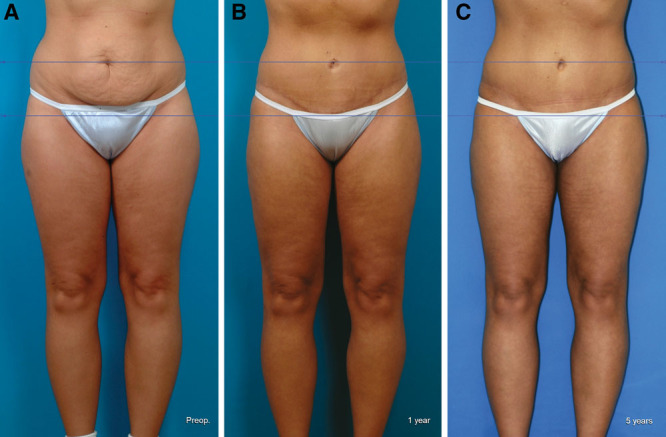
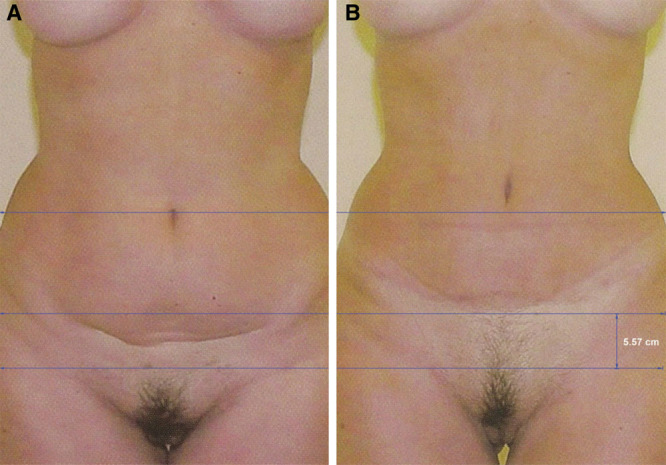
Conclusions: Lipoabdominoplasty may be performed safely, so that patients may benefit from both modalities. The seroma rate is reduced by avoiding electrodissection, making Scarpa fascia preservation a moot point. A deep fascial repair keeps the abdominoplasty scar within the bikini line. Deep venous thrombosis and other complications may be minimized with precautions that do not include anticoagulation.
Conflict of interest statement
Disclosure: The author has no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the author.
Figures







References
-
- Swanson E. Prospective clinical study reveals significant reduction in triglyceride level and white cell count after liposuction and abdominoplasty and no change in cholesterol levels. Plast Reconstr Surg. 2011;128:182e–197e. discussion 198e–200e. - PubMed
-
- Swanson E. Prospective outcome study of 360 patients treated with liposuction, lipoabdominoplasty, and abdominoplasty. Plast Reconstr Surg. 2012;129:965–978. discussion 979–980. - PubMed
-
- Swanson E. Photographic measurements in 301 cases of liposuction and abdominoplasty reveal fat reduction without redistribution. Plast Reconstr Surg. 2012;130:311e–322e. discussion 323e–324e. - PubMed
-
- Swanson E. Prospective study of lidocaine, bupivacaine and epinephrine levels and blood loss in patients undergoing liposuction and abdominoplasty. Plast Reconstr Surg. 2012;130:702–722. discussion 723–725. - PubMed
-
- Heller JB, Teng E, Knoll BI, et al. Outcome analysis of combined lipoabdominoplasty versus conventional abdominoplasty. Plast Reconstr Surg. 2008;121:1821–1829. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources