

Histological and Ultrastructural Effects of Ultrasound-induced Cavitation on Human Skin Adipose Tissue
- PMID: 25289235
- PMCID: PMC4174158
- DOI: 10.1097/GOX.0b013e3182a7f222
Histological and Ultrastructural Effects of Ultrasound-induced Cavitation on Human Skin Adipose Tissue
Abstract
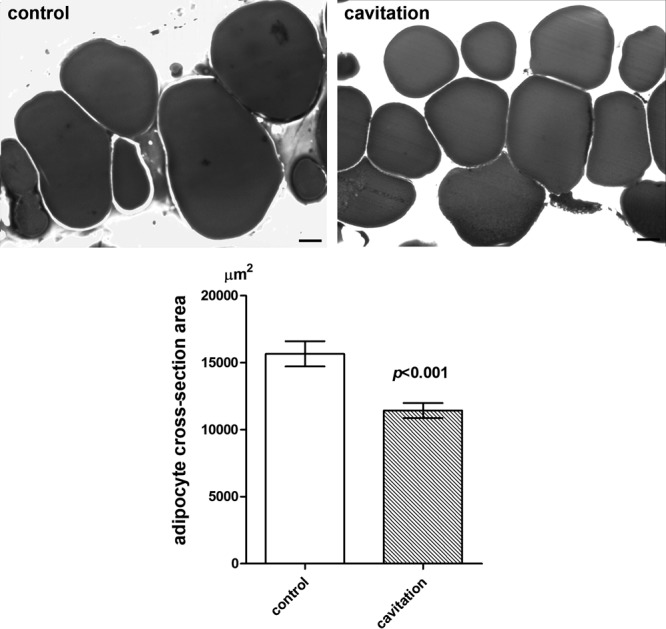
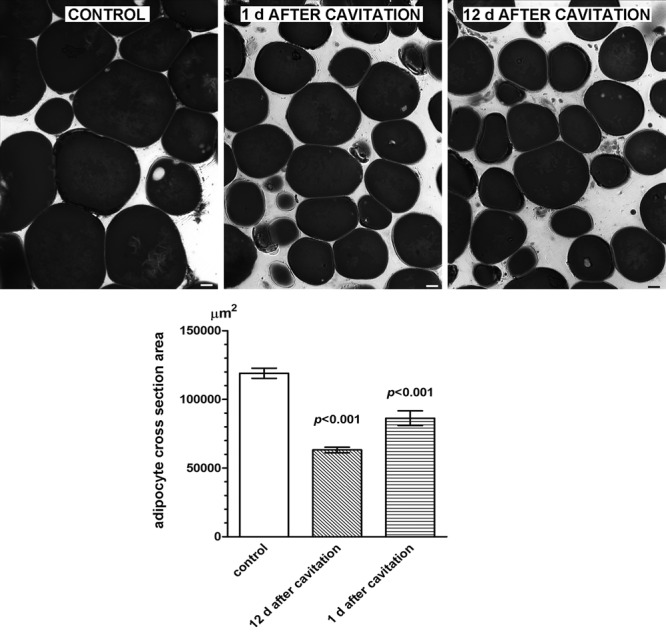
Background: In aesthetic medicine, the most promising techniques for noninvasive body sculpturing purposes are based on ultrasound-induced fat cavitation. Liporeductive ultrasound devices afford clinically relevant subcutaneous fat pad reduction without significant adverse reactions. This study aims at evaluating the histological and ultrastructural changes induced by ultrasound cavitation on the different cell components of human skin.
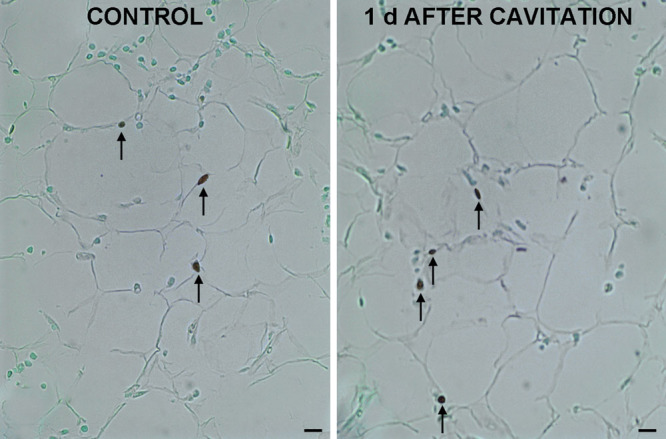
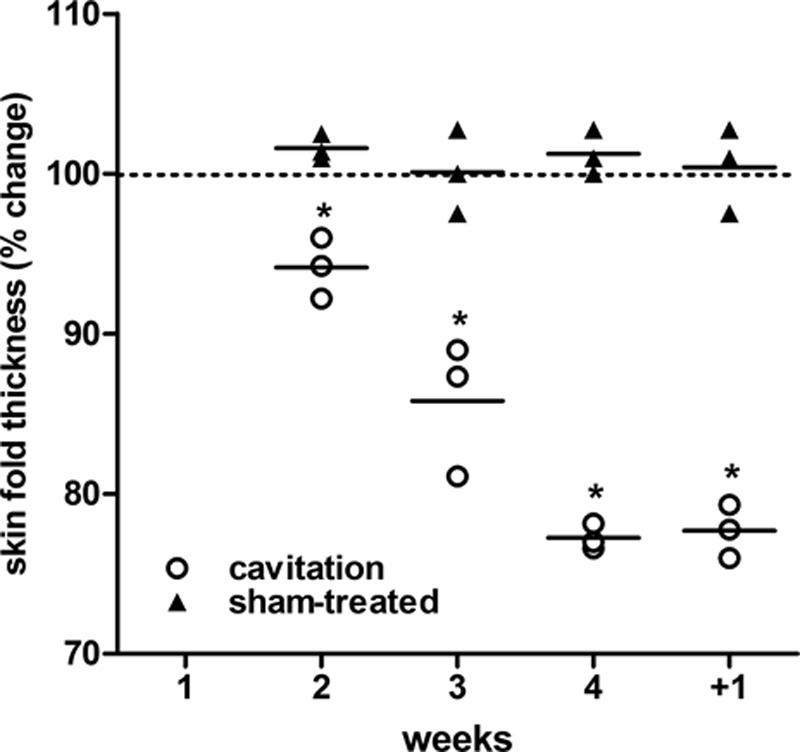
Methods: Control and ultrasound-treated ex vivo abdominal full-thickness skin samples and skin biopsies from patients pretreated with or without ultrasound cavitation were studied histologically, morphometrically, and ultrastructurally to evaluate possible changes in adipocyte size and morphology. Adipocyte apoptosis and triglyceride release were also assayed. Clinical evaluation of the effects of 4 weekly ultrasound vs sham treatments was performed by plicometry.
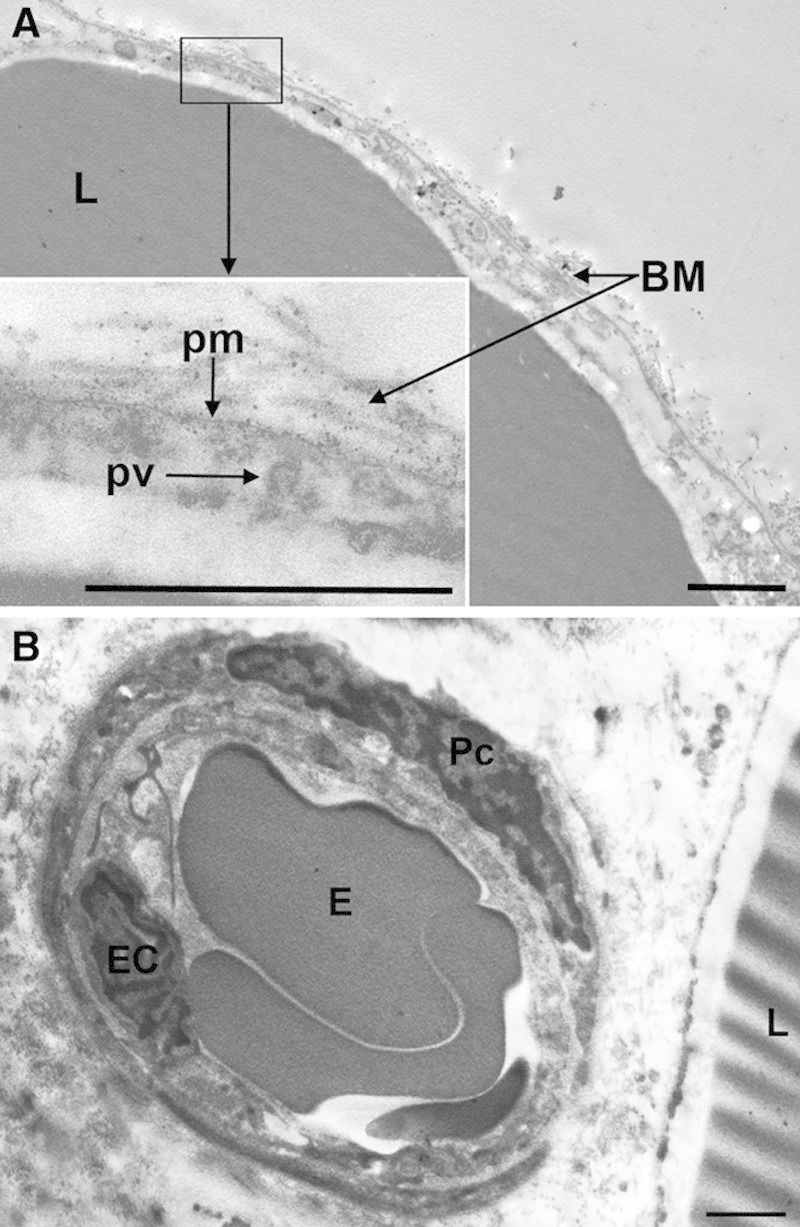
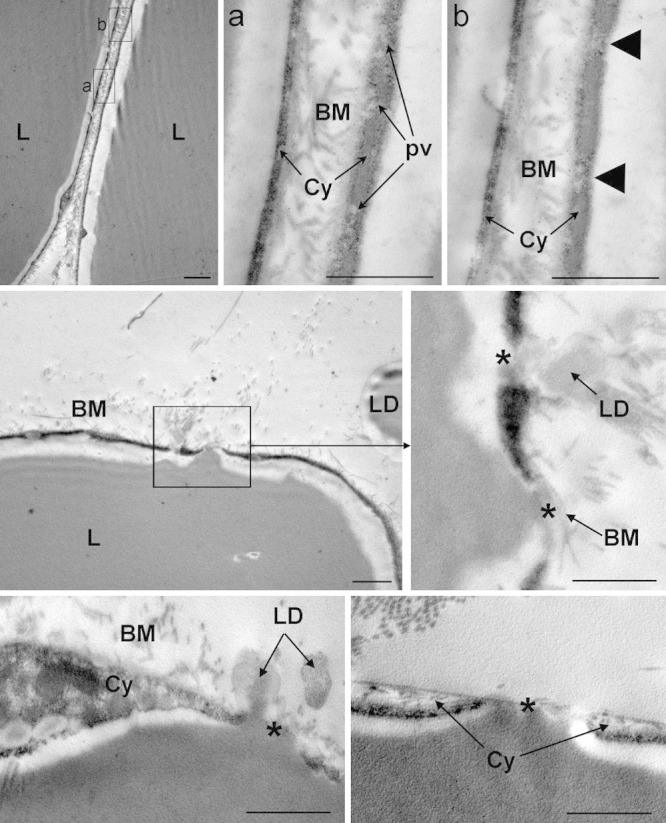
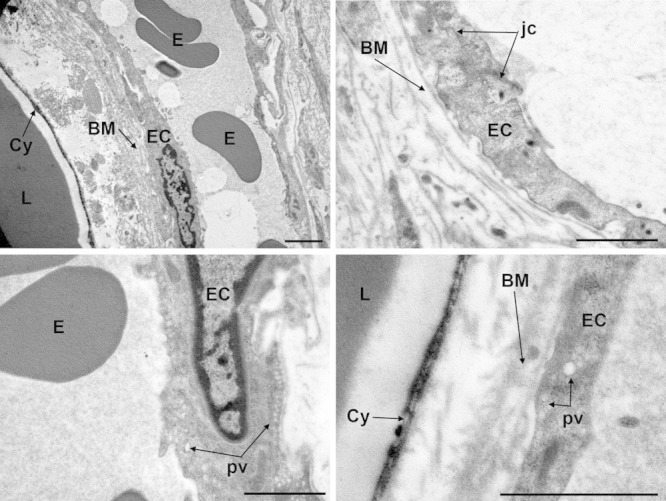
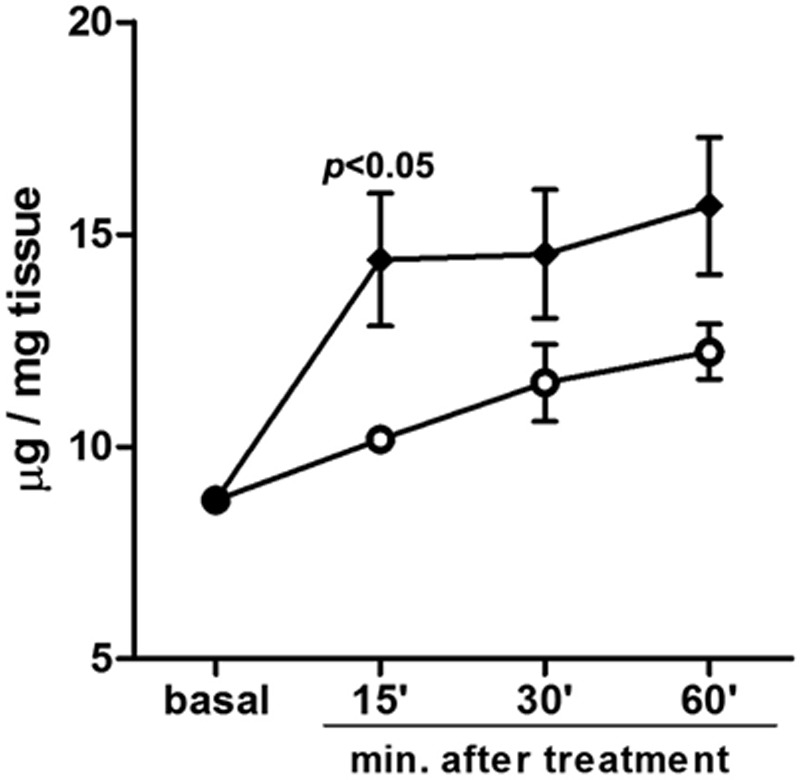
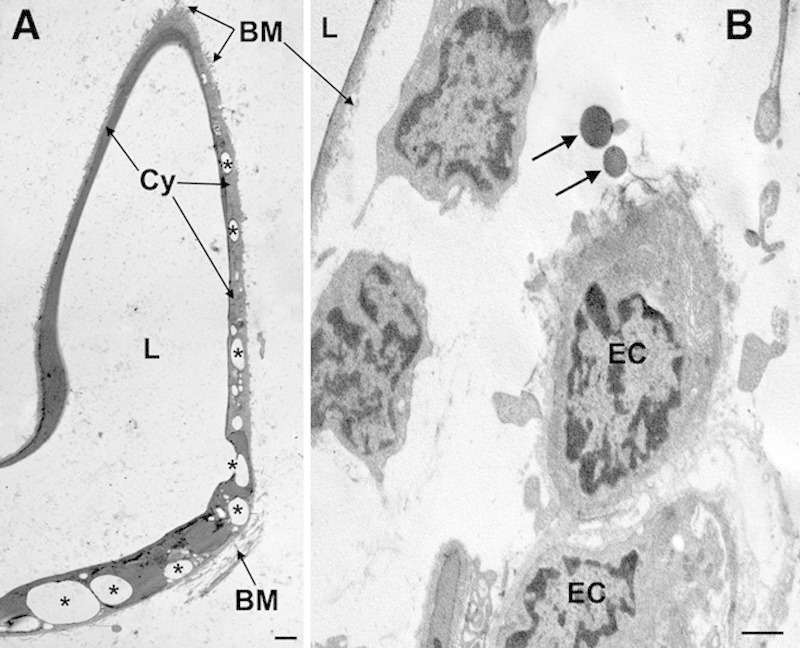
Results: Compared with the sham-treated control samples, ultrasound cavitation induced a statistically significant reduction in the size of the adipocytes (P < 0.001), the appearance of micropores and triglyceride leakage and release in the conditioned medium (P < 0.05 at 15 min), or adipose tissue interstitium, without appreciable changes in microvascular, stromal, and epidermal components and in the number of apoptotic adipocytes. Clinically, the ultrasound treatment caused a significant reduction of abdominal fat.
Conclusions: This study further strengthens the current notion that noninvasive transcutaneous ultrasound cavitation is a promising and safe technology for localized reduction of fat and provides experimental evidence for its specific mechanism of action on the adipocytes.
Figures
References
-
- Housman TS, Lawrence N, Mellen BG, et al. The safety of liposuction: results of a national survey. Dermatol Surg. 2002;28:971–978. - PubMed
-
- Coleman KM, Coleman WP, III, Benchetrit A. Non-invasive, external ultrasonic lipolysis. Semin Cutan Med Surg. 2009;28:263–267. - PubMed
-
- Neira R, Arroyave J, Ramirez H, et al. Fat liquefaction: effect of low-level laser energy on adipose tissue. Plast Reconstr Surg. 2002;110:912–922; discussion 923. - PubMed
-
- Jackson RF, Dedo DD, Roche GC, et al. Low-level laser therapy as a non-invasive approach for body contouring: a randomized controlled study. Lasers Surg Med. 2009;41:799–809. - PubMed
-
- Manuskiatti W, Wachirakaphan C, Lektrakul N, et al. Circumference reduction and cellulite treatment with a Tri-Polar radiofrequency device: a pilot study. J Eur Acad Dermatol Venereol. 2009;23:820–827. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources