

Paralytic ectropion treatment with lateral periosteal flap canthoplasty and introduction of the ectropion severity score
- PMID: 25289344
- PMCID: PMC4174080
- DOI: 10.1097/GOX.0000000000000084
Paralytic ectropion treatment with lateral periosteal flap canthoplasty and introduction of the ectropion severity score
Abstract
Background: Paralytic ectropion patients suffer from impairment of function and appearance of the lower eyelid and are at high risk of developing an exposure keratitis. A canthoplasty procedure can reduce the horizontal eyelid laxity and elevate the lower eyelid. We used a periosteal flap from the outer orbit to create a new canthal ligament. This study investigates the long-term outcomes of this technique.
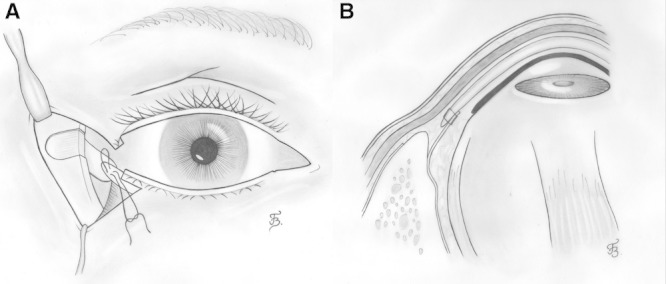
Methods: Cross-sectional outcome study in which 30 cases of paralytic ectropion are treated with a lateral periosteal flap canthoplasty after adequate eyelid shortening. At the desired canthal height, a periosteal flap from the outer temporal orbital rim is mobilized around the rim and sutured in a double-breasted fashion to a tarsal strip. Effect of the operation is measured by comparing preoperative and postoperative photographs for signs of ectropion. For this purpose, a new photograph-based scoring method [the Ectropion Severity Score (ESS)] was developed and evaluated.
Results: The ESS proved to be reliable and sensitive to the presence of ectropion. Significant improvement of the ectropion sequelae was measured after a mean follow-up period of 2 years. In 3 cases (13%), a revision procedure was necessary because of relapse of lower eyelid sagging after a mean time of 1.9 years. In these cases, the periosteal flap could be reused.
Conclusions: The ESS is a useful instrument to score the severity of paralytic ectropion. The periosteal flap canthoplasty is an effective procedure, with durable results in paralytic ectropion patients. The same periosteal flap can be used in a revision procedure.
Figures



References
-
- Goldberg RA. Review of prophylactic lateral canthopexy in lower blepharoplasties. Arch Facial Plast Surg. 2003;5:272–275. - PubMed
-
- Anderson RL, Gordy DD. The tarsal strip procedure. Arch Ophthalmol. 1979;97:2192–2196. - PubMed
-
- Moe KS, Linder T. The lateral transorbital canthopexy for correction and prevention of ectropion: report of a procedure, grading system, and outcome study. Arch Facial Plast Surg. 2000;2:9–15. - PubMed
-
- Bergeron CM, Moe KS. The evaluation and treatment of lower eyelid paralysis. Facial Plast Surg. 2008;24:231–241. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources