

Excess non-psychiatric hospitalizations among employees with mental disorders: a 10-year prospective study of the GAZEL cohort
- PMID: 25289581
- PMCID: PMC4402031
- DOI: 10.1111/acps.12341
Excess non-psychiatric hospitalizations among employees with mental disorders: a 10-year prospective study of the GAZEL cohort
Abstract
Objective: To examine whether non-psychiatric hospitalizations rates were higher in those with mental disorders.
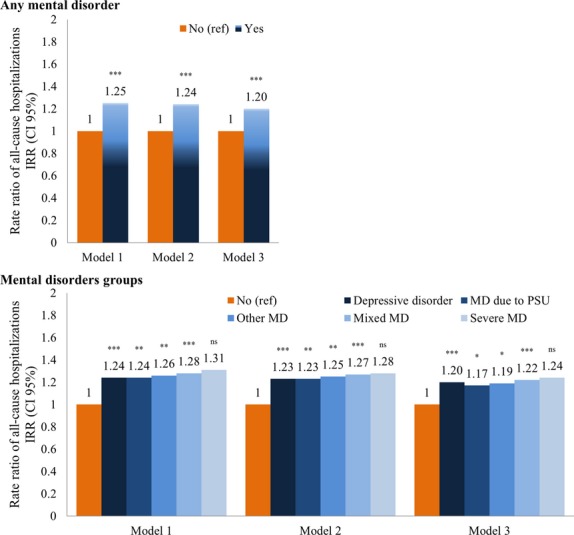
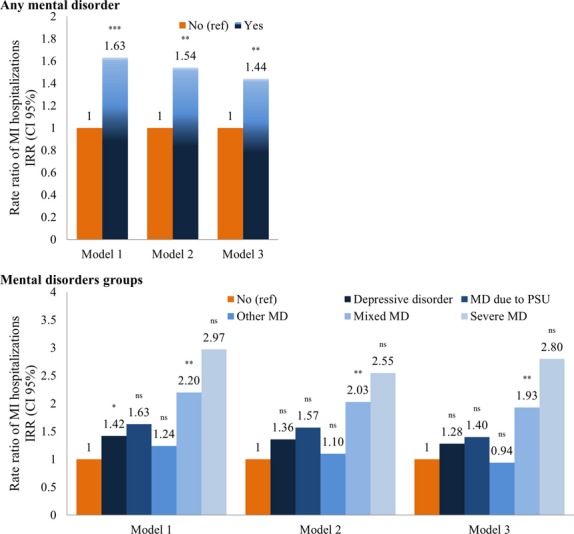
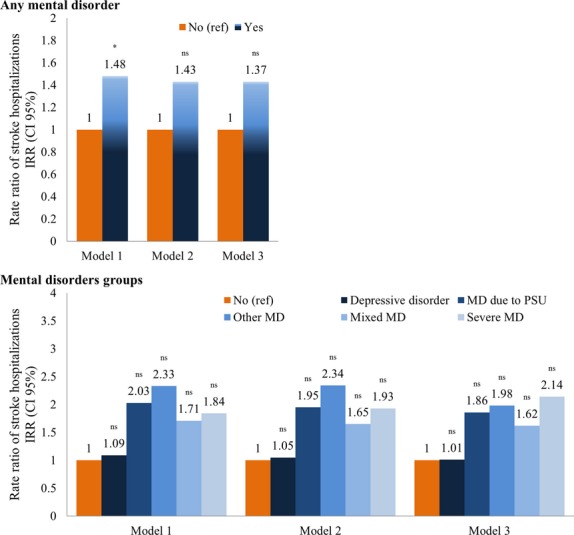
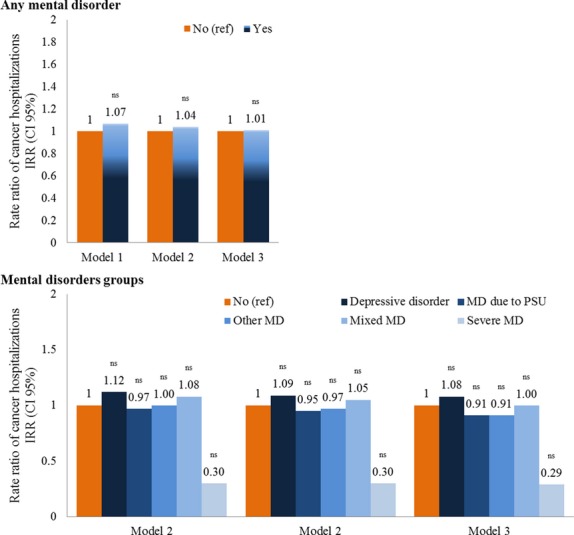
Method: In a cohort of 15,811 employees, aged 35-50 years in 1989, mental disorder status was defined from 1989 to 2000. Hospitalizations for all-causes, myocardial infarction (MI), stroke, and cancer, were recorded yearly from 2001 to 2011. Negative binomial regression models were used to estimate hospitalization rates over the follow-up.
Results: After controlling for baseline sociodemographic factors, health-related behaviors, self-rated health, and self-reported medical conditions, participants with a mental disorder had significantly higher rates of all-cause hospitalization [incidence rate ratio, IRR=1.20 (95%, 1.14-1.26)], as well as hospitalization due to MI [IRR=1.44 (95%, 1.12-1.85)]. For stroke, the IRR did not reach statistical significance [IRR=1.37 (95%, 0.95-1.99)] and there was no association with cancer [IRR=1.01 (95%, 0.86-1.19)]. A similar trend was observed when mental disorders groups were considered (no mental disorder, depressive disorder, mental disorders due to psychoactive substance use, other mental disorders, mixed mental disorders, and severe mental disorder).
Conclusion: In this prospective cohort of employees with stable employment as well as universal access to healthcare, we found participants with mental disorders to have higher rates of non-psychiatric hospitalizations.
Keywords: chronic disease; healthcare; hospitalizations; mental disorders; prospective study.
© 2014 The Authors. Acta Psychiatrica Scandinavica Published by John Wiley & Sons Ltd.
Figures
Comment in
-
Are there any lessons to be learnt from psychiatric epidemiology?Acta Psychiatr Scand. 2015 Apr;131(4):240-1. doi: 10.1111/acps.12346. Epub 2014 Oct 8. Acta Psychiatr Scand. 2015. PMID: 25294310 No abstract available.
References
-
- Harris EC, Barraclough B. Excess mortality of mental disorder. Br J Psychiatry. 1998;173:11–53. - PubMed
-
- Brown S, Inskip H, Barraclough B. Causes of the excess mortality of schizophrenia. Br J Psychiatry. 2000;177:212–217. - PubMed
-
- Fagiolini A, Goracci A. The effects of undertreated chronic medical illnesses in patients with severe mental disorders. J Clin Psychiatry. 2009;70(Suppl. 3):22–29. - PubMed
-
- Saha S, Chant D, McGrath J. A systematic review of mortality in schizophrenia: is the differential mortality gap worsening over time? Arch Gen Psychiatry. 2007;64:1123–1131. - PubMed
-
- Amaddeo F, Barbui C, Perini G, Biggeri A, Tansella M. Avoidable mortality of psychiatric patients in an area with a community-based system of mental health care. Acta Psychiatr Scand. 2007;115:320–325. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
