

Cost-effectiveness of HIV drug resistance testing to inform switching to second line antiretroviral therapy in low income settings
- PMID: 25290340
- PMCID: PMC4188574
- DOI: 10.1371/journal.pone.0109148
Cost-effectiveness of HIV drug resistance testing to inform switching to second line antiretroviral therapy in low income settings
Erratum in
- PLoS One. 2014;9(12):e115079. Magubu, Travor [corrected to Mabugu, Travor]
Abstract
Background: To guide future need for cheap resistance tests for use in low income settings, we assessed cost-effectiveness of drug resistance testing as part of monitoring of people on first line ART - with switching from first to second line ART being conditional on NNRTI drug resistance mutations being identified.
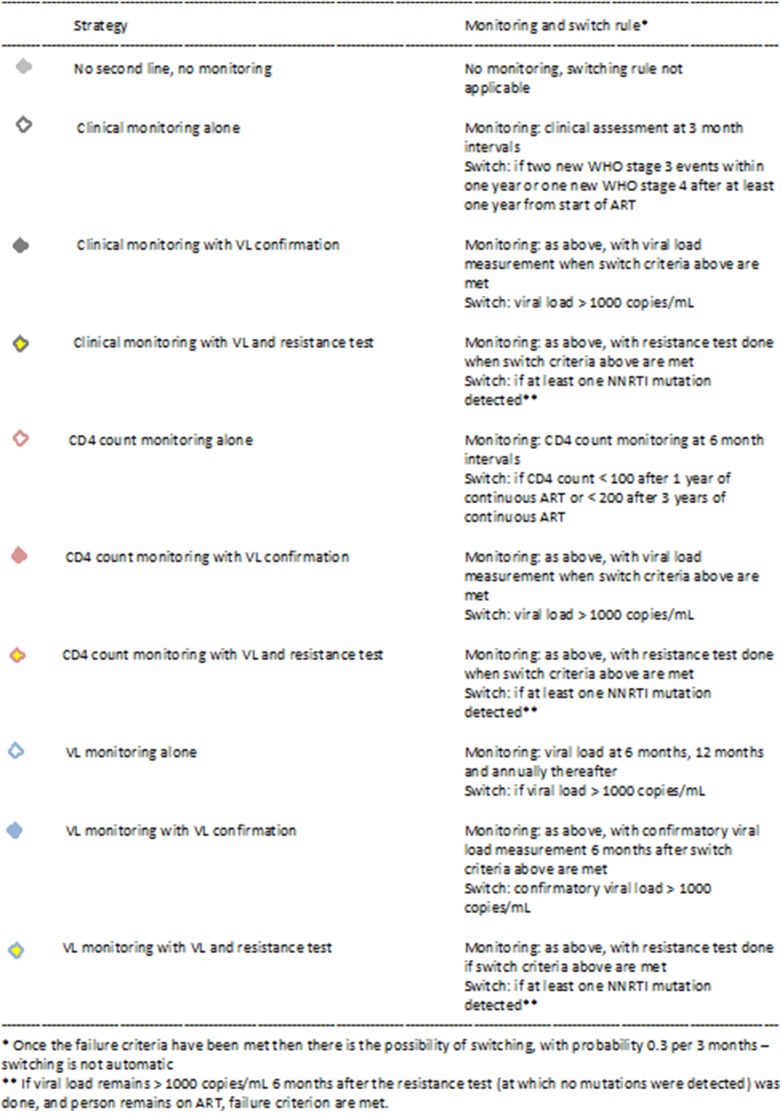
Methods: An individual level simulation model of HIV transmission, progression and the effect of ART which accounts for adherence and resistance development was used to compare outcomes of various potential monitoring strategies in a typical low income setting in sub-Saharan Africa. Underlying monitoring strategies considered were based on clinical disease, CD4 count or viral load. Within each we considered a strategy in which no further measures are performed, one with a viral load measure to confirm failure, and one with both a viral load measure and a resistance test. Predicted outcomes were assessed over 2015-2025 in terms of viral suppression, first line failure, switching to second line regimen, death, HIV incidence, disability-adjusted-life-years averted and costs. Potential future low costs of resistance tests ($30) were used.
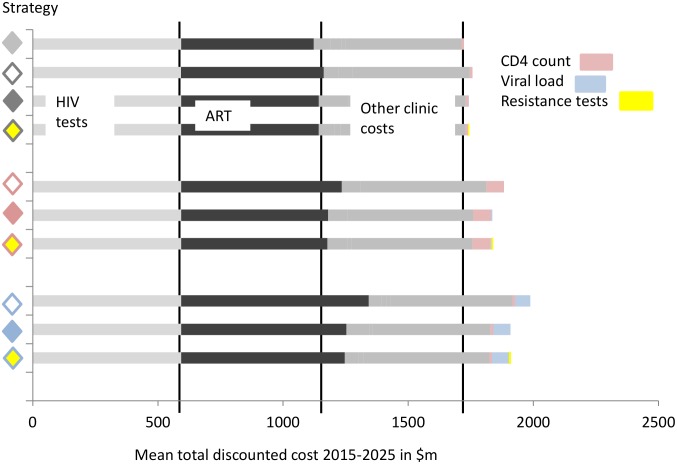
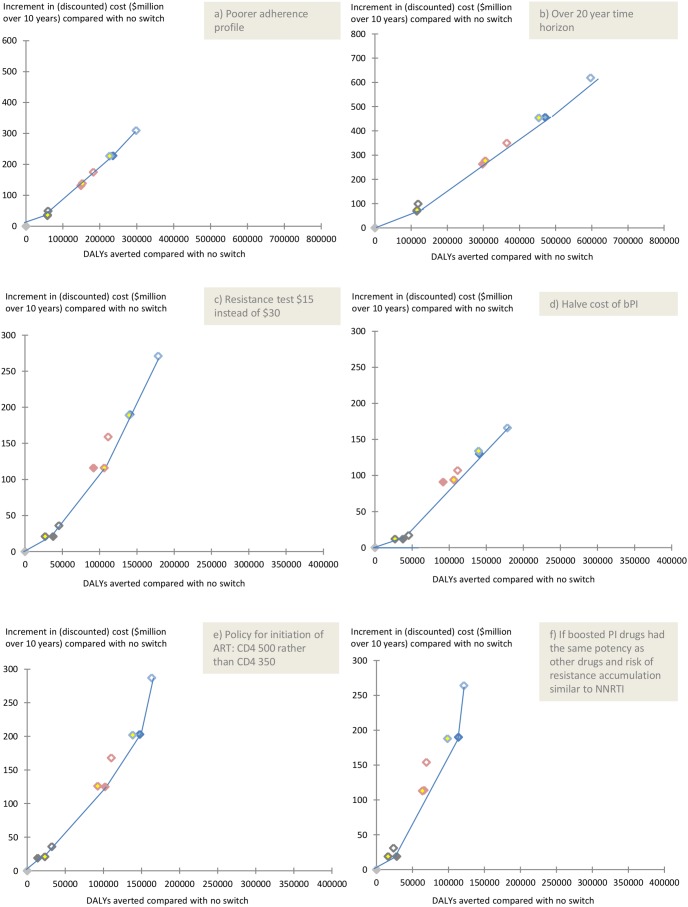
Results: The most effective strategy, in terms of DALYs averted, was one using viral load monitoring without confirmation. The incremental cost-effectiveness ratio for this strategy was $2113 (the same as that for viral load monitoring with confirmation). ART monitoring strategies which involved resistance testing did not emerge as being more effective or cost effective than strategies not using it. The slightly reduced ART costs resulting from use of resistance testing, due to less use of second line regimens, was of similar magnitude to the costs of resistance tests.
Conclusion: Use of resistance testing at the time of first line failure as part of the decision whether to switch to second line therapy was not cost-effective, even though the test was assumed to be very inexpensive.
Conflict of interest statement
Figures


References
-
- WHO (2013) Global update on HIV treatment 2013: Results, impact and opportunities.
-
- WHO (2013) Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. Recommendations for a public health approach. - PubMed
-
- Gupta R, Hill A, Sawyer AW, Pillay D (2008) Emergence of drug resistance in HIV type 1-infected patients after receipt of first-line highly active antiretroviral therapy: a systematic review of clinical trials. Clin Infect Dis 47: 712–722. - PubMed
-
- Johnston V, Cohen K, Wiesner L, Morris L, Ledwaba J, et al. (2014) Viral suppression following switch to second-line antiretroviral therapy: associations with nucleoside reverse transcriptase inhibitor resistance and subtherapeutic drug concentrations prior to switch. J Infect Dis 209: 711–720. - PMC - PubMed
-
- Williams I, Churchill D, Anderson J, Boffito M, Bower M, et al. (2012) British HIV Association guidelines for the treatment of HIV-1-positive adults with antiretroviral therapy 2012. HIV Med 13 Suppl 2: 1–85. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
