

Causes and consequences of adult laryngotracheal stenosis
- PMID: 25290987
- PMCID: PMC4562418
- DOI: 10.1002/lary.24956
Causes and consequences of adult laryngotracheal stenosis
Abstract
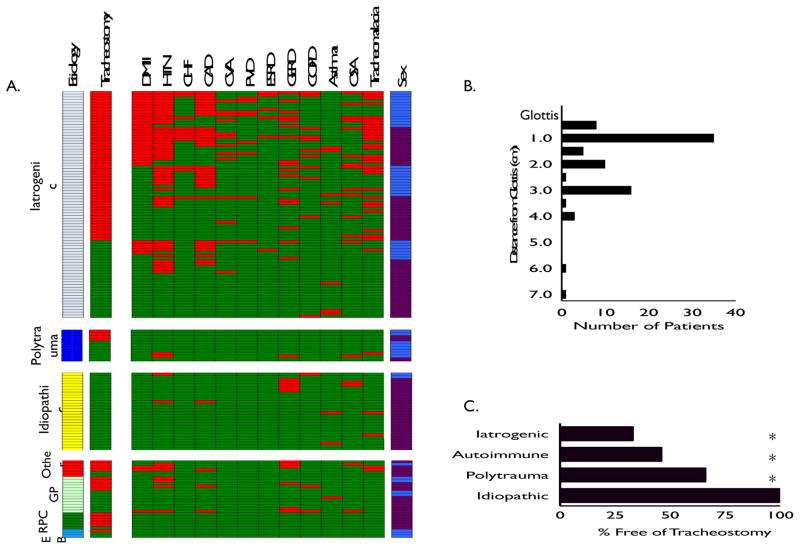
Objectives/hypothesis: Laryngotracheal stenosis (LTS) is largely considered a structural entity, defined on anatomic terms (i.e., percent stenosis, distance from vocal folds, overall length). This has significant implications for identifying at-risk populations, devising systems-based preventive strategies, and promoting patient-centered treatment. The present study was undertaken to test the hypothesis that LTS is heterogeneous with regard to etiology, natural history, and clinical outcome.
Study design: Retrospective cohort study of consecutive adult tracheal stenosis patients from 1998 to 2013.
Methods: Subjects diagnosed with laryngotracheal stenosis (ICD-9: 478.74, 519.19) between January 1, 1998, and January 1, 2013, were identified. Patient characteristics (age, gender, race, follow-up duration) and comorbidities were extracted. Records were reviewed for etiology of stenosis, treatment approach, and surgical dates. Stenosis morphology was derived from intraoperative measurements. The presence of tracheostomy at last follow-up was recorded.
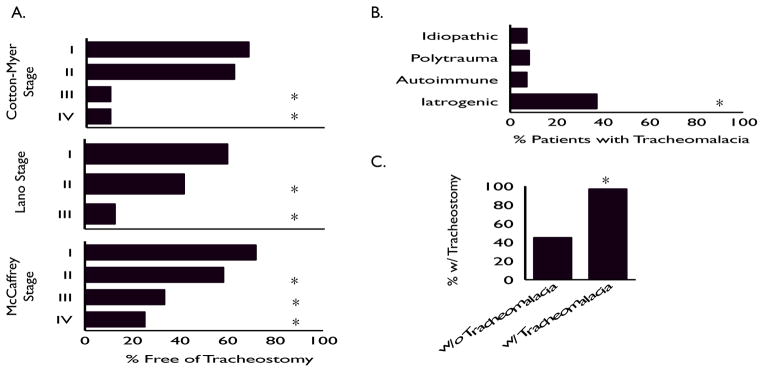
Results: One hundred and fifty patients met inclusion criteria. A total of 54.7% had an iatrogenic etiology, followed by idiopathic (18.5%), autoimmune (18.5%), and traumatic (8%). Tracheostomy dependence differed based on etiology (P < 0.001). Significantly more patients with iatrogenic (66%) and autoimmune (54%) etiologies remained tracheostomy-dependent compared to traumatic (33%) or idiopathic (0%) groups. On multivariate regression analysis, each additional point on Charlson Comorbidity Index was associated with a 67% increased odds of tracheostomy dependence (odds ratio 1.67; 95% confidence interval 1.04-2.69; P = 0.04).
Conclusions: Laryngotracheal stenosis is not a homogeneous clinical entity. It has multiple distinct etiologies that demonstrate disparate rates of long-term tracheostomy dependence. Understanding the mechanism of injury and contribution of comorbid illnesses is critical to systems-based preventive strategies and patient-centered treatment.
Level of evidence: 4.
Keywords: Tracheal stenosis; intubation; laryngotracheal stenosis; subglottic; tracheostomy.
© 2014 The American Laryngological, Rhinological and Otological Society, Inc.
Conflict of interest statement
Figures
References
-
- Nouraei SA, Singh A, Patel A, Ferguson C, Howard DJ, Sandhu GS. Early endoscopic treatment of acute inflammatory airway lesions improves the outcome of postintubation airway stenosis. The Laryngoscope. 2006;116:1417–1421. - PubMed
-
- Institute of Medicine (U.S.). Committee on Quality of Health Care in America. Crossing the quality chasm : a new health system for the 21st century. Washington, D.C: National Academy Press; 2001.
-
- Cotton RT. Pediatric laryngotracheal stenosis. Journal of pediatric surgery. 1984;19:699–704. - PubMed
-
- Lano CF, Jr, Duncavage JA, Reinisch L, Ossoff RH, Courey MS, Netterville JL. Laryngotracheal reconstruction in the adult: a ten year experience. The Annals of otology, rhinology, and laryngology. 1998;107:92–97. - PubMed
-
- McCaffrey TV. Classification of laryngotracheal stenosis. The Laryngoscope. 1992;102:1335–1340. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
