

Neonatal morbidity associated with shoulder dystocia maneuvers
- PMID: 25291256
- PMCID: PMC4467960
- DOI: 10.1016/j.ajog.2014.10.001
Neonatal morbidity associated with shoulder dystocia maneuvers
Abstract
Objective: We sought to examine neonatal morbidity associated with different maneuvers used among term patients who experience a shoulder dystocia.
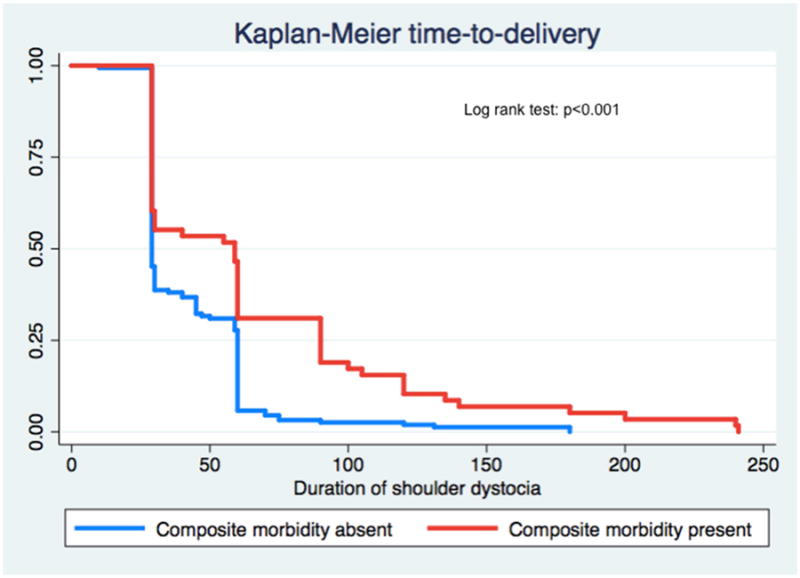
Study design: We conducted a retrospective cohort study of all women who experienced a clinically diagnosed shoulder dystocia at term requiring obstetric maneuvers at a single tertiary care hospital from 2005 through 2008. We excluded women with major fetal anomaly, intrauterine death, multiple gestation, and preterm. Women exposed to Rubin maneuver, Wood's screw maneuver, or delivery of the posterior arm were compared to women delivered by McRoberts/suprapubic pressure only, which served as the reference group. The primary outcome was a composite morbidity of neonatal injury (defined as clavicular or humeral fracture or brachial plexus injury) and neonatal depression (defined as Apgar <7 at 5 minutes, arterial cord pH <7.1, continuous positive airway pressure use, intubation, or respiratory distress). Logistic regression was used to adjust for nulliparity and duration of shoulder dystocia, defined as time from delivery of fetal head to delivery of shoulders.
Results: Among the 231 women who met inclusion criteria, 135 were delivered by McRoberts/suprapubic pressure alone (57.9%), 83 women were exposed to Rubin maneuver, 53 women were exposed to Wood's screw, and 36 women were exposed to delivery of posterior arm. Individual maneuvers were not associated with composite morbidity, neonatal injury, or neonatal depression after adjusting for nulliparity and duration of shoulder dystocia.
Conclusion: We found no association between shoulder dystocia maneuvers and neonatal morbidity after adjusting for duration, a surrogate for severity. Our results demonstrate that clinicians should utilize the maneuver most likely to result in successful delivery.
Keywords: neonatal morbidity; shoulder dystocia; shoulder dystocia maneuvers.
Copyright © 2015 Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure: The authors report no conflicts of interest.
Figures
Similar articles
-
Maternal body mass index, maneuvers, and neonatal morbidity associated with shoulder dystocia.Am J Obstet Gynecol. 2025 Jun;232(6):570.e1-570.e7. doi: 10.1016/j.ajog.2024.10.036. Epub 2024 Nov 7. Am J Obstet Gynecol. 2025. PMID: 39515446
-
Obstetric maneuvers for shoulder dystocia and associated fetal morbidity.Am J Obstet Gynecol. 1998 Jun;178(6):1126-30. doi: 10.1016/s0002-9378(98)70312-6. Am J Obstet Gynecol. 1998. PMID: 9662290
-
Maternal and neonatal complications of shoulder dystocia with a focus on obstetric maneuvers: A case-control study of 1103 deliveries.Acta Obstet Gynecol Scand. 2024 Oct;103(10):1965-1974. doi: 10.1111/aogs.14780. Epub 2024 Jan 26. Acta Obstet Gynecol Scand. 2024. PMID: 38276972 Free PMC article.
-
[Shoulder dystocia: Guidelines for clinical practice--Short text].J Gynecol Obstet Biol Reprod (Paris). 2015 Dec;44(10):1303-10. doi: 10.1016/j.jgyn.2015.09.053. Epub 2015 Nov 2. J Gynecol Obstet Biol Reprod (Paris). 2015. PMID: 26541561 Review. French.
-
Shoulder dystocia: guidelines for clinical practice from the French College of Gynecologists and Obstetricians (CNGOF).Eur J Obstet Gynecol Reprod Biol. 2016 Aug;203:156-61. doi: 10.1016/j.ejogrb.2016.05.047. Epub 2016 May 30. Eur J Obstet Gynecol Reprod Biol. 2016. PMID: 27318182 Review.
Cited by
-
Shoulder Dystocia: A Comprehensive Literature Review on Diagnosis, Prevention, Complications, Prognosis, and Management.J Pers Med. 2024 May 30;14(6):586. doi: 10.3390/jpm14060586. J Pers Med. 2024. PMID: 38929807 Free PMC article. Review.
-
Shoulder dystocia and composite adverse outcomes for the maternal-neonatal dyad.Am J Obstet Gynecol MFM. 2021 Jul;3(4):100359. doi: 10.1016/j.ajogmf.2021.100359. Epub 2021 Mar 20. Am J Obstet Gynecol MFM. 2021. PMID: 33757935 Free PMC article.
-
Anal sphincter injury in vaginal deliveries complicated by shoulder dystocia.Int Urogynecol J. 2018 Mar;29(3):377-381. doi: 10.1007/s00192-017-3351-2. Epub 2017 May 18. Int Urogynecol J. 2018. PMID: 28523399
-
Simulation in shoulder dystocia: does it change outcomes?BMJ Simul Technol Enhanc Learn. 2018 Mar 29;5(2):91-95. doi: 10.1136/bmjstel-2017-000280. eCollection 2019. BMJ Simul Technol Enhanc Learn. 2018. PMID: 35519828 Free PMC article.
-
Shoulder dystocia: incidence, mechanisms, and management strategies.Int J Womens Health. 2018 Nov 9;10:723-732. doi: 10.2147/IJWH.S175088. eCollection 2018. Int J Womens Health. 2018. PMID: 30519118 Free PMC article. Review.
References
-
- Shoulder dystocia. ACOG Practice Bulletin No. 40, November 2002. American College of Obstetricians and Gynecologists. Obstet Gynecol. 2002;100:1045–50. - PubMed
-
- Gherman RB, Ouzounian JG, Goodwin TM. Obstetric maneuvers for shoulder dystocia and associated fetal morbidity. Am J Obstet Gynecol. 1998;178:1126–30. - PubMed
-
- Cunningham FG, Williams JW. Williams obstetrics. 22nd. New York (NY): McGraw-Hill Professional; 2005.
-
- McFarland MB, Langer O, Piper JM, Berkus MD. Perinatal outcome and the type and number of maneuvers in shoulder dystocia. Int J Gynecol Obstet. 1996;55:219–24. - PubMed
-
- Gherman RB, Goodwin TM, Souter I, Neumann K, Ouzounian JG, Paul RH. The McRoberts' maneuver for the alleviation of shoulder dystocia: How successful is it? Am J Obstet Gynecol. 1997;176:656–61. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
