

Rotational thromboelastometry predicts thromboembolic complications after major non-cardiac surgery
- PMID: 25292221
- PMCID: PMC4200117
- DOI: 10.1186/s13054-014-0549-2
Rotational thromboelastometry predicts thromboembolic complications after major non-cardiac surgery
Abstract
Introduction: Thromboembolic complications contribute substantially to perioperative morbidity and mortality. Routine laboratory tests do not detect patients with acquired or congenital hypercoagulability who may be at increased risk of perioperative thromboembolism. Rotational thromboelastometry (ROTEM) is a digitized modification of conventional thromboelastography that is stable and technically easy to use. We designed a prospective observational study to evaluate whether preoperative ROTEM can identify patients at increased risk for postoperative thromboembolic complications after major non-cardiac surgery.
Methods: Preoperative ROTEM analysis using extrinsic rotational thromboelastometry (EXTEM), intrinsic rotational thromboelastometry (INTEM), and fibrinogen rotational thromboelastometry (FIBTEM) activators was performed on 313 patients undergoing major non-cardiac surgery. Patients' medical records were reviewed after discharge for results of standard coagulation studies - partial thromboplastin time (PTT), international normalized ratio (INR), platelet count - and evidence of thromboembolic complications during their hospital stay. A thromboembolic complication was defined as a new arterial or deep venous thrombosis, catheter thrombosis, or pulmonary embolism diagnosed by ultrasound or spiral chest computed tomography.
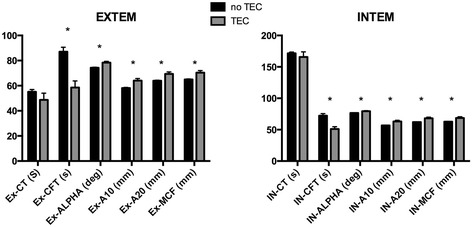
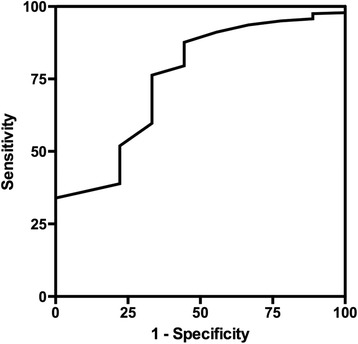
Results: Ten patients developed postoperative thromboembolic complications, of whom 9 had received standard prophylaxis with subcutaneous enoxaparin or heparin. There was no indication of by PTT, INR, or platelet count. Preoperative EXTEM and INTEM activators that assess fibrin clot formation and platelet interaction indicated that these patients had significantly lower clot formation time (CFT) and significantly higher alpha angle (α) and maximum clot firmness (MCF), compared to patients without thromboembolic complications. There was no significant difference for any parameter using FIBTEM activator, which excludes platelet interaction. Receiver operating characteristic (ROC) curves were constructed for these variables. INTEM clot firmness at 10 min (A10) was the best predictor of thromboembolic complications, with an ROC area under the curve of 0.751.
Conclusions: Our results indicate that preoperative ROTEM assays that include fibrin clot and platelet interaction may detect patients at increased risk for postoperative thromboembolic complications after major non-cardiac surgery. Future studies need to evaluate the clinical utility and cost effectiveness of preoperative ROTEM and better define the association between ROTEM values and specific hypercoagulable conditions.
Figures
Comment in
-
Rotational thrombelastometry: a step forward to safer patient care?Crit Care. 2014 Dec 26;18(6):706. doi: 10.1186/s13054-014-0706-7. Crit Care. 2014. PMID: 25672525 Free PMC article.
References
-
- Kakkar VV, Cohen AT, Edmonson RA, Phillips MJ, Cooper DJ, Das SK, Maher KT, Sanderson RM, Ward VP, Kakkar S. Low molecular weight versus standard heparin for prevention of venous thromboembolism after major abdominal surgery. The Thromboprophylaxis Collaborative Group. Lancet. 1993;341:259–265. doi: 10.1016/0140-6736(93)92614-Y. - DOI - PubMed
-
- Lowe GD, Haverkate F, Thompson SG, Turner RM, Bertina RM, Turpie AG, Mannucci PM. Prediction of deep vein thrombosis after elective hip replacement surgery by preoperative clinical and haemostatic variables: the ECAT DVT Study. European Concerted Action on Thrombosis. Thromb Haemost. 1999;81:879–886. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
