

Changes in erectile dysfunction over time in relation to Framingham cardiovascular risk in the Boston Area Community Health (BACH) Survey
- PMID: 25293632
- PMCID: PMC4304913
- DOI: 10.1111/jsm.12715
Changes in erectile dysfunction over time in relation to Framingham cardiovascular risk in the Boston Area Community Health (BACH) Survey
Abstract
Introduction: Erectile dysfunction (ED) is associated with cardiovascular disease (CVD); however, the association between change in ED status over time and future underlying CVD risk is unclear.
Aim: The aim of this study was to investigate the association between change in ED status and Framingham CVD risk, as well change in Framingham risk.
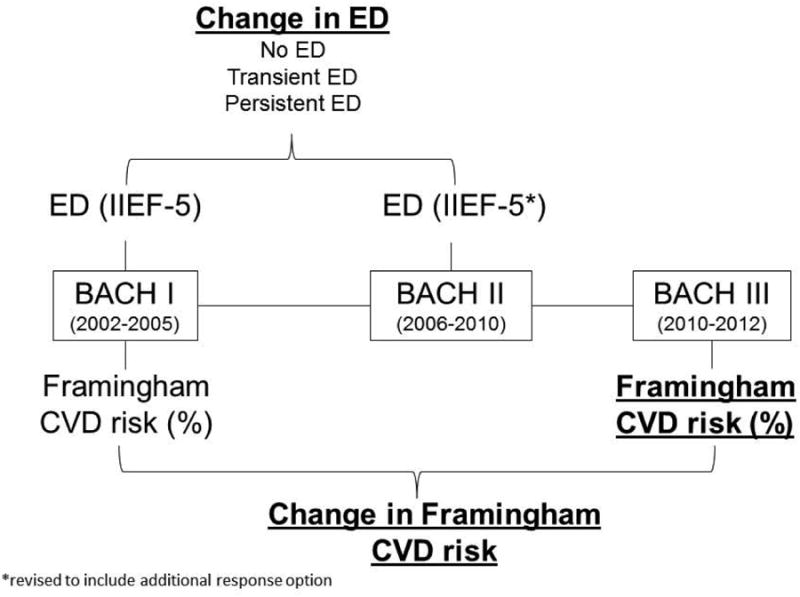
Methods: We studied 965 men free of CVD in the Boston Area Community Health (BACH) Survey, a longitudinal cohort study with three assessments. ED was assessed with the five-item International Index of Erectile Function at BACH I (2002-2005) and BACH II (2007-2010) and classified as no ED/transient ED/persistent ED. CVD risk was assessed with 10-year Framingham CVD risk algorithm at BACH I and BACH III (2010-2012). Linear regression models controlled for baseline age, socio-demographic and lifestyle factors, as well as baseline Framingham risk. Models were also stratified by age (≥/< 50 years).
Main outcome measures: Framingham CVD risk and change in Framingham CVD risk were the main outcome measures.
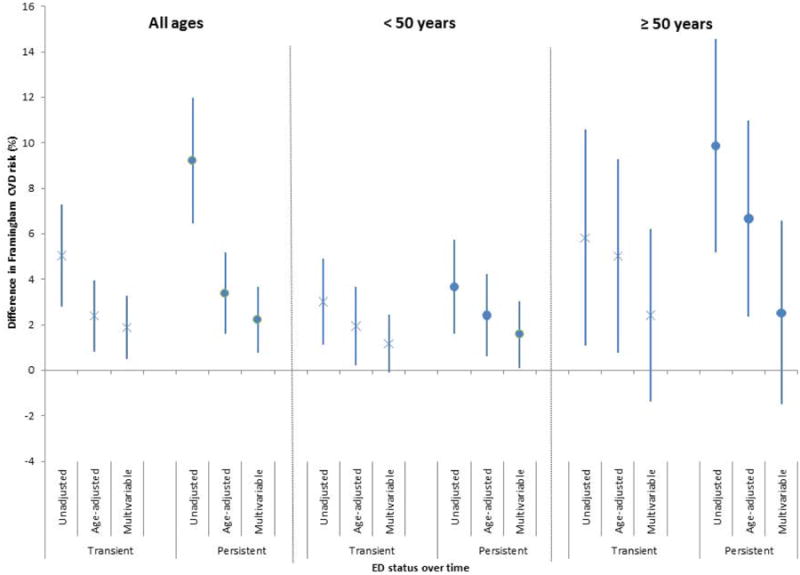
Results: Transient and persistent ED was significantly associated with increased Framingham risk and change in risk over time in univariate and age-adjusted models. In younger men, persistent ED was associated with a Framingham risk that was 1.58 percentage points higher (95% confidence interval [CI]: 0.11, 3.06) and in older men, a Framingham risk that was 2.54 percentage points higher (95% CI: -1.5, 6.59), compared with those without ED. Change in Framingham risk over time was also associated with transient and persistent ED in men <50 years, but not in older men.
Conclusions: Data suggest that even after taking into account other CVD risk factors, transient and persistent ED is associated with Framingham CVD risk and a greater increase in Framingham risk over time, particularly in younger men. Findings further support clinical assessment of CVD risk in men presenting with ED, especially those under 50 years.
Keywords: Changes in Erectile Function; Male; Prospective Cohort; Sexual Dysfunction.
© 2014 International Society for Sexual Medicine.
Conflict of interest statement
Conflict of Interest: None
Figures

References
-
- Selvin E, Burnett AL, Platz EA. Prevalence and risk factors for erectile dysfunction in the US. Am J Med. 2007;120(2):151–7. - PubMed
-
- Feldman HA, Johannes CB, Derby CA, Kleinman KP, Mohr BA, Araujo AB, et al. Erectile dysfunction and coronary risk factors: prospective results from the Massachusetts male aging study. Prev Med. 2000;30(4):328–38. - PubMed
-
- Saigal CS, Wessells H, Pace J, Schonlau M, Wilt TJ. Predictors and prevalence of erectile dysfunction in a racially diverse population. Arch Intern Med. 2006;166(2):207–12. - PubMed
-
- Schouten BW, Bohnen AM, Bosch JL, Bernsen RM, Deckers JW, Dohle GR, et al. Erectile dysfunction prospectively associated with cardiovascular disease in the Dutch general population: results from the Krimpen Study. Int J Impot Res. 2008;20(1):92–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
