

Electrophysiologic substrate in congenital Long QT syndrome: noninvasive mapping with electrocardiographic imaging (ECGI)
- PMID: 25294783
- PMCID: PMC4245321
- DOI: 10.1161/CIRCULATIONAHA.114.011359
Electrophysiologic substrate in congenital Long QT syndrome: noninvasive mapping with electrocardiographic imaging (ECGI)
Abstract
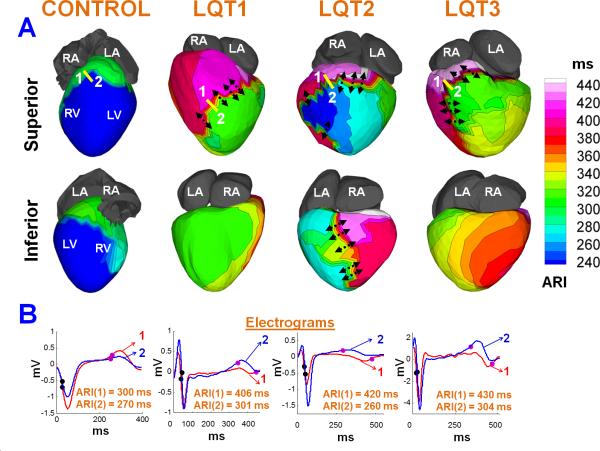
Background: Congenital Long QT syndrome (LQTS) is an arrhythmogenic disorder that causes syncope and sudden death. Although its genetic basis has become well-understood, the mechanisms whereby mutations translate to arrhythmia susceptibility in the in situ human heart have not been fully defined. We used noninvasive ECG imaging to map the cardiac electrophysiological substrate and examine whether LQTS patients display regional heterogeneities in repolarization, a substrate that promotes arrhythmogenesis.
Methods and results: Twenty-five subjects (9 LQT1, 9 LQT2, 5 LQT3, and 2 LQT5) with genotype and phenotype positive LQTS underwent ECG imaging. Seven normal subjects provided control. Epicardial maps of activation, recovery times, activation-recovery intervals, and repolarization dispersion were constructed. Activation was normal in all patients. However, recovery times and activation-recovery intervals were prolonged relative to control, indicating delayed repolarization and abnormally long action potential duration (312±30 ms versus 235±21 ms in control). Activation-recovery interval prolongation was spatially heterogeneous, with repolarization gradients much steeper than control (119±19 ms/cm versus 2.0±2.0 ms/cm). There was variability in steepness and distribution of repolarization gradients between and within LQTS types. Repolarization gradients were steeper in symptomatic patients (130±27 ms/cm in 12 symptomatic patients versus 98±19 ms/cm in 13 asymptomatic patients; P<0.05).
Conclusions: LQTS patients display regions with steep repolarization dispersion caused by localized action potential duration prolongation. This defines a substrate for reentrant arrhythmias, not detectable by surface ECG. Steeper dispersion in symptomatic patients suggests a possible role for ECG imaging in risk stratification.
Keywords: ECG imaging; arrhythmia; electrophysiology; imaging, diagnostic; long-QT syndrome.
© 2014 American Heart Association, Inc.
Figures


Comment in
-
New insights into the arrhythmogenic substrate of the long QT syndrome.Circulation. 2014 Nov 25;130(22):1929-30. doi: 10.1161/CIRCULATIONAHA.114.013232. Epub 2014 Oct 7. Circulation. 2014. PMID: 25294784 Free PMC article. No abstract available.
References
-
- Roden DM, Balser JR, George AL, Anderson ME. Cardiac ion channels. Annu Rev Physiol. 2002;64:431–475. - PubMed
-
- Rautaharju PM, Surawicz B, Gettes LS, Bailey JJ, Childers R, Deal BJ, Gorgels A, Hancock EW, Josephson M, Kligfield P, Kors JA, Macfarlane P, Mason JW, Mirvis DM, Okin P, Pahlm O, van Herpen G, Wagner GS, Wellens H. American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; American College of Cardiology Foundation; Heart Rhythm Society. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part IV: the ST segment, T and U waves, and the QT interval: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society: endorsed by the International Society for Computerized Electrocardiology. J Am Coll Cardiol. 2009;53:982–991. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
