

Review
doi: 10.1155/2014/864369.
Epub 2014 Sep 8.
Multidetector computer tomography: evaluation of blunt chest trauma in adults
Affiliations
- PMID: 25295188
- PMCID: PMC4175749
- DOI: 10.1155/2014/864369
Item in Clipboard
Review
Multidetector computer tomography: evaluation of blunt chest trauma in adults
Radiol Res Pract.
2014.
Abstract
Imaging plays an essential part of chest trauma care. By definition, the employed imaging technique in the emergency setting should reach the correct diagnosis as fast as possible. In severe chest blunt trauma, multidetector computer tomography (MDCT) has become part of the initial workup, mainly due to its high sensitivity and diagnostic accuracy of the technique for the detection and characterization of thoracic injuries and also due to its wide availability in tertiary care centers. The aim of this paper is to review and illustrate a spectrum of characteristic MDCT findings of blunt traumatic injuries of the chest including the lungs, mediastinum, pleural space, and chest wall.
Figures
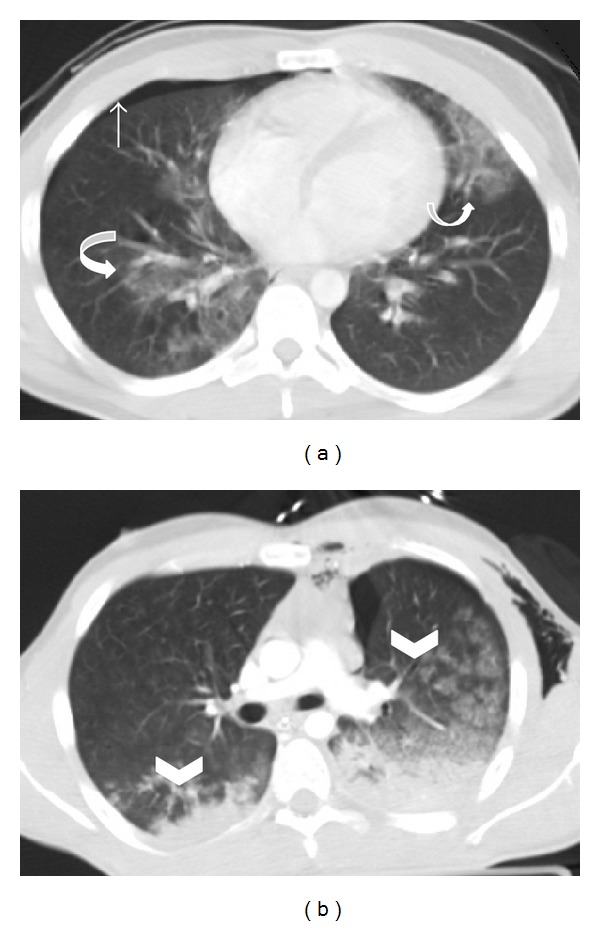
Bilateral pulmonary contusion. Axial MDCT in lung window reveals (a) ill-defined nonsegmental areas of “ground glass” attenuation in middle lobe, right inferior lobe, and lingula in a polytraumatized patient, consistent with bilateral contusion focus (curved arrows). Also note a small right pneumothorax (straight arrow). Axial MDCT of another patient (b) shows “ground glass” lung contusions (arrowheads) and bilateral nonsegmental air space consolidations with a posterior distribution due to blood filling of the alveolar spaces.

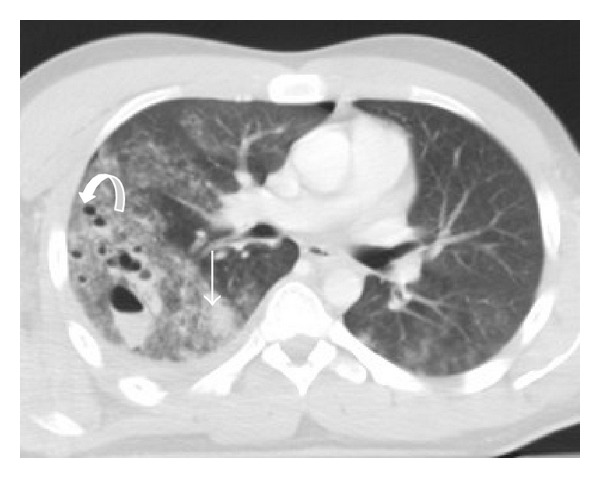
Pulmonary contusion and hemothorax in a patient who fell down of his bike. Axial MDCT in lung window at the level of left cardiac chamber shows right lower lung contusion (thin arrow) associated with ipsilateral hemothorax (thick arrow).
Pulmonary lacerations. Axial MDCT in lung window at the level of pulmonary trunk. Multiple focus of pulmonary lacerations can be depicted, some of them are filled with air (pneumatocele, curved arrow), others filled with blood (hematocele-straight arrow), and some filled with both, making an air-liquid level (pneumo-hematocele, arrowhead). Surrounding pulmonary contusions are appreciated. Associated left pulmonary contusions and a small right pneumothorax are also depicted.

Tracheal rupture. Coronal reconstruction of axial MDCT in lung window. An extensive subcutaneous emphysema, bilateral pneumothorax, and pneumomediastinum are observed. Close attention to the tracheal wall depicted a small leak of air to the mediastinum (arrow).

Polytraumatized patient who was hit by a car. Axial MDCT after intravenous contrast administration, at the level of aortic arch, demonstrates mediastinal hemorrhage (thin arrow) and left anterior chest muscle wall hematoma (pectoralis major, thick arrow).

Thoracic aortic pseudoaneurysm in the context of blunt chest trauma. Sagittal reconstruction of arterial phase MDCT demonstrates an abnormal contour of the thoracic aorta. A sacculation filled with iodinated contrast material involving the anterior aspect of transition of the aortic arch with the descending aorta, immediately after the emergency of the left subclavian artery, consistent with aortic pseudoaneurysm (arrow).

Hemopericardium and bilateral hemothorax. Postcontrast axial MDCT of a polytraumatized patient reveals a pericardial (curved arrow) and a bilateral pleural effusion (straight arrows), with high attenuation consistent with fresh blood content.

Pneumopericardium. A thin line of air is appreciated between the pericardium layers (arrow). Bilateral parenchymal contusions were also present.
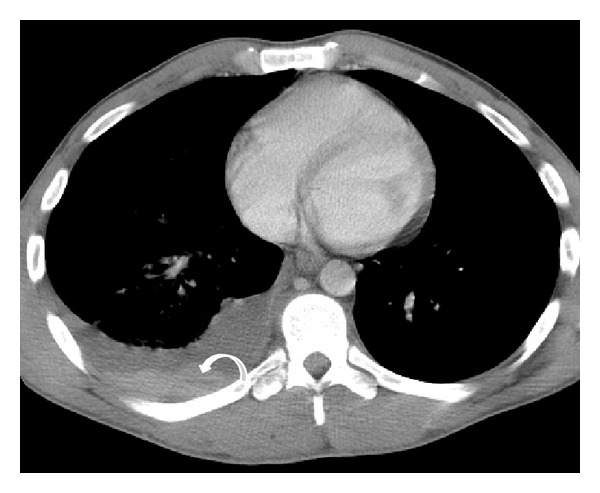
Right hemothorax with the “hematocrit sign.” Postcontrast axial MDCT at the level of ventricular chambers demonstrates a right pleural effusion with a liquid-liquid level (curved arrow), giving an aspect of layered effusion, consistent with right hemothorax with different degrees of blood coagulation (“hematocrit sign”).

Right hemothorax and pneumothorax. Postcontrast axial MCDT shows a right hemopneumothorax creating an air-liquid level (arrow).
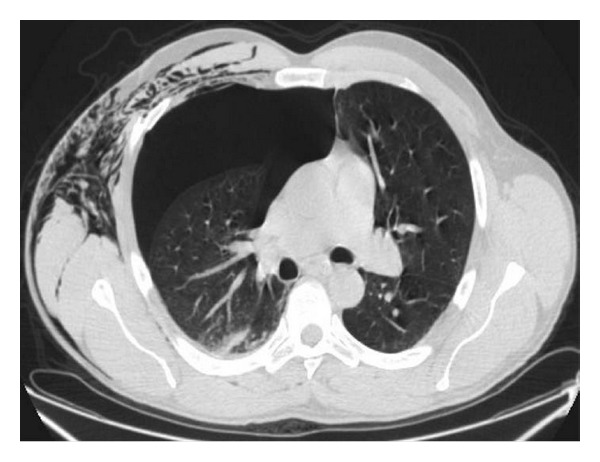
Tension pneumothorax. Axial MDCT in lung window at the level of the pulmonary trunk shows increased volume of the right hemithorax due to a large pneumothorax. This finding reduces the ipsilateral pulmonary volume and shifts the mediastinum to the left. A small contusion focus in the posterior segment of the right upper lobe and subcutaneous emphysema are also seen. This is an indication for immediate chest drainage.

Rib fracture. Axial MDCT in bone window at the level of pulmonary trunk clearly demonstrates a fracture bone line of 8th posterior right arch associated with ipsilateral hemothorax.

Rib fractures in 2 polytraumatized patients. Coronal MDCT in bone window (a) in a case of “flail chest” with four displaced rib fractures (straight arrows) in three consecutive right costal arches and in one left costal arc. Note the associated pulmonary contusions. Another patient (b) presenting with multiple left rib fractures (arrows), shown with oblique sagittal volume-rendering reconstruction.

Sternum fracture in two different patients. Axial MDCT (bone window) in patient one (a) shows a complete sternum fracture at the level of the body, without displacement of the fragments (arrow). Axial MDCT (b) and sagittal reconstruction in bone window (c) in a second patient show a displaced sternal body fracture (arrows). A small retrosternal hematoma is also seen (b).
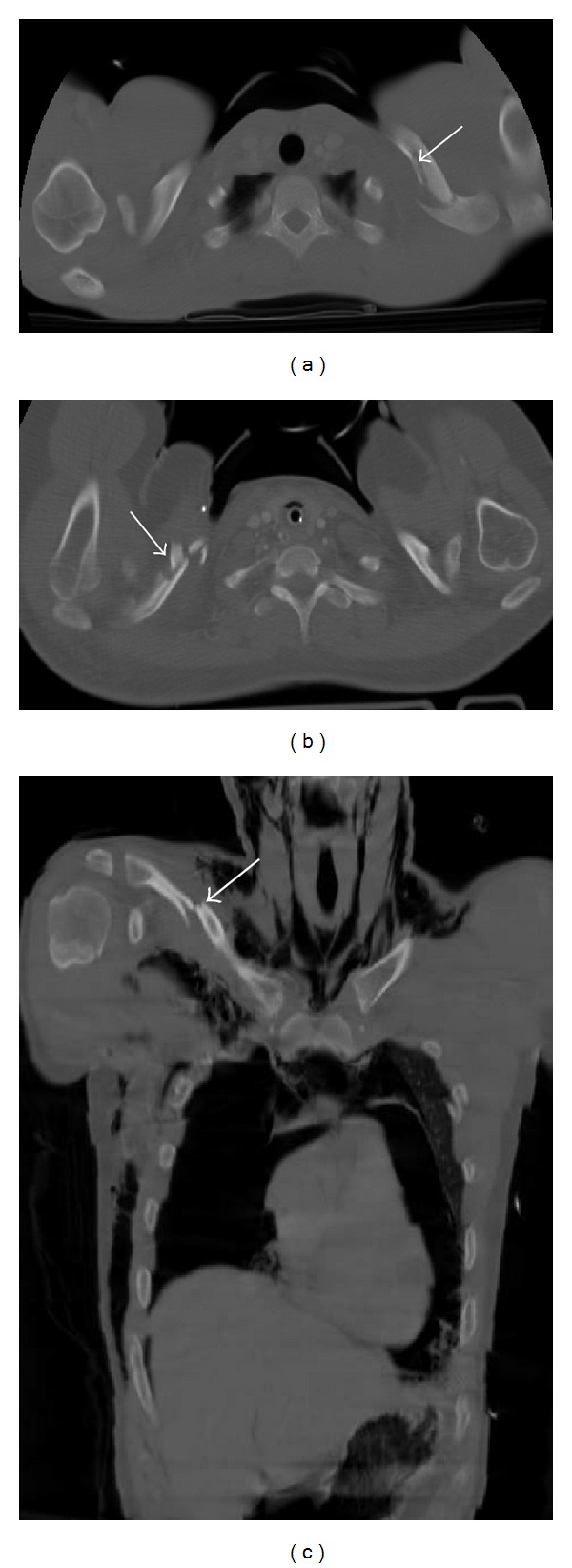
Three cases of clavicle fractures. Axial MDCT reconstruction in bone window ((a), (b)) and coronal reconstruction in bone window (c). A two-fracture line is seen in the left clavicle (a); a comminuted fracture is seen in the right clavicle, with multiple fragments (b); and a middle third fracture with dislocation is seen in the right clavicle (c). In (c) there are associated left anterior costal arc fracture, right pneumothorax, pneumomediastinum, and subcutaneous emphysema.
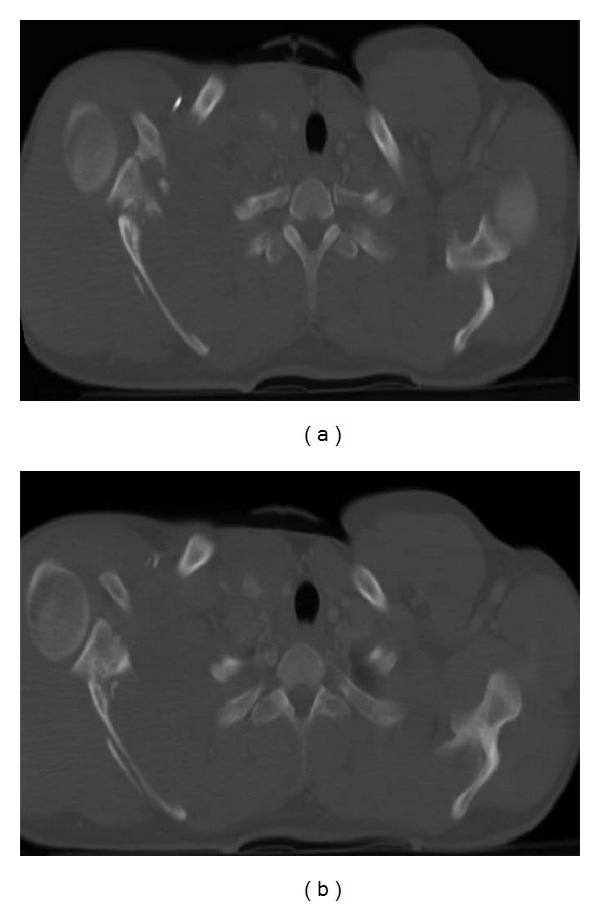
Right scapular fracture. Axial MDCT in bone window ((a), (b)). Comminuted right scapular fracture involving the scapular neck and spine is clearly observed.
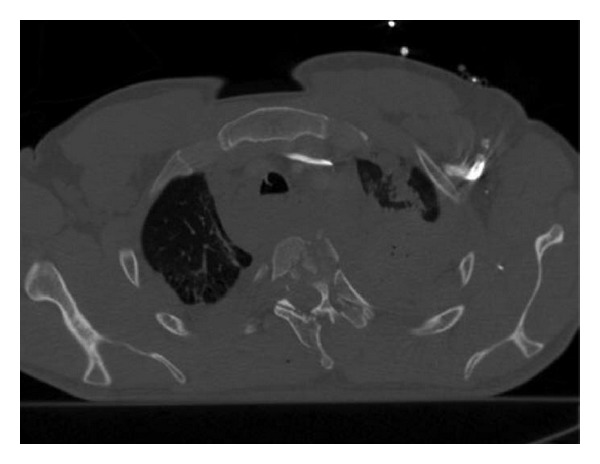
Thoracic vertebral fracture in a patient who suffered a car crash. Axial MDCT in bone window. A comminuted thoracic vertebral fracture is depicted with multiple fragments of the body and spinous processes of the third thoracic vertebra. Hemomediastinum, hemothorax, and pulmonary contusions are also associated.
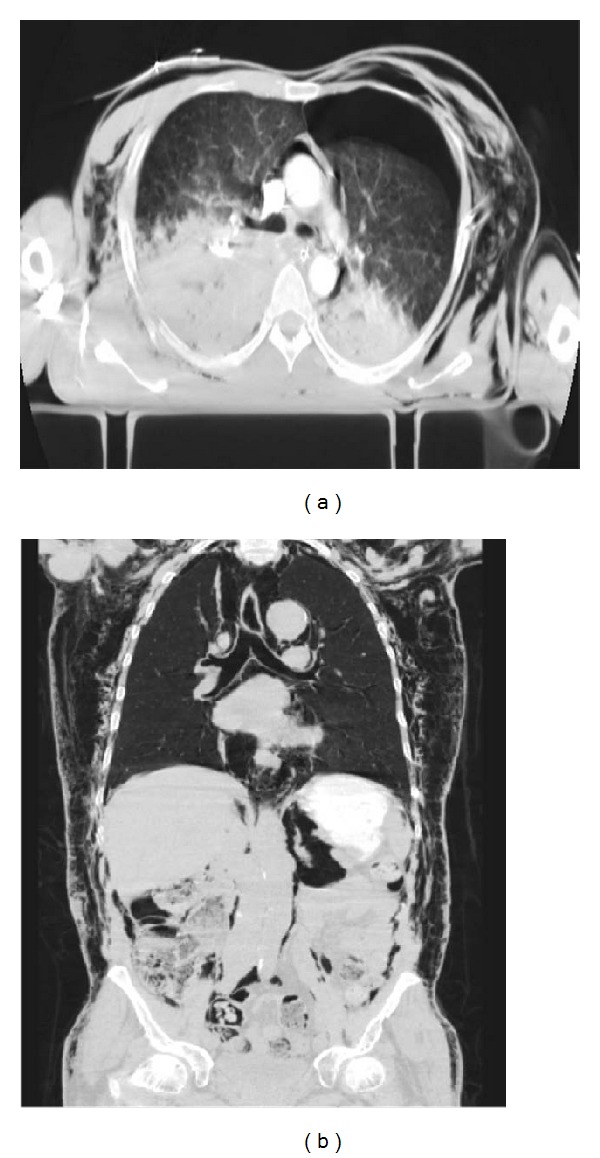
Subcutaneous emphysema. Axial MDCT (a) and coronal reconstruction (b) in lung window. An extensive subcutaneous emphysema is observed. A pneumomediastinum and retropneumoperitoneum are also associated.
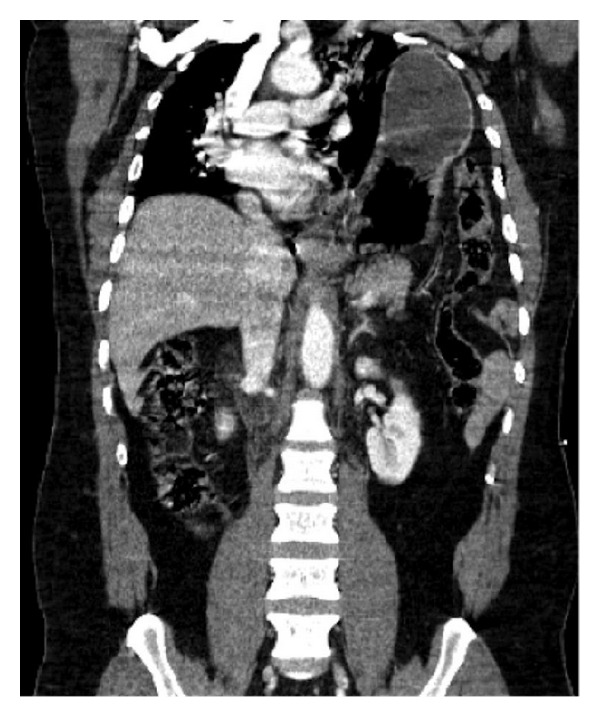
Signs of rupture of the diaphragm. Coronal MDCT reconstruction. A massive left diaphragmatic hernia with herniation of the stomach and left colon content is seen in a patient who suffered a car accident. It decreases left pulmonary volume and shifts the mediastinum towards right.
Similar articles
-
Blunt traumatic injuries of the lung parenchyma, pleura, thoracic wall, and intrathoracic airways: multidetector computer tomography imaging findings.Emerg Radiol. 2007 Oct;14(5):297-310. doi: 10.1007/s10140-007-0651-8. Epub 2007 Jul 11. Emerg Radiol. 2007. PMID: 17623115 Review.
-
Imaging of Combat-Related Thoracic Trauma - Blunt Trauma and Blast Lung Injury.Mil Med. 2018 Mar 1;183(3-4):e89-e96. doi: 10.1093/milmed/usx033. Mil Med. 2018. PMID: 29514343
-
Thoracic wall trauma-misdiagnosed lesions on radiographs and usefulness of ultrasound, multidetector computed tomography and magnetic resonance imaging.Quant Imaging Med Surg. 2017 Aug;7(4):384-397. doi: 10.21037/qims.2017.08.02. Quant Imaging Med Surg. 2017. PMID: 28932697 Free PMC article. Review.
-
Chest wall, lung, and pleural space trauma.Radiol Clin North Am. 2006 Mar;44(2):213-24, viii. doi: 10.1016/j.rcl.2005.10.006. Radiol Clin North Am. 2006. PMID: 16500204 Review.
-
[A contribution of multidetector computed tomography to indications for chest wall stabilisation in multiple rib fractures].Acta Chir Orthop Traumatol Cech. 2011;78(3):258-61. Acta Chir Orthop Traumatol Cech. 2011. PMID: 21729644 Czech.
Cited by
-
Diagnostic accuracy of a commercially available deep-learning algorithm in supine chest radiographs following trauma.Br J Radiol. 2022 Jun 1;95(1134):20210979. doi: 10.1259/bjr.20210979. Epub 2022 Mar 24. Br J Radiol. 2022. PMID: 35271382 Free PMC article.
-
Posterior membranous tracheal injury during mckeown oesophagectomy. A case report with literature review.Front Oncol. 2025 May 9;15:1560437. doi: 10.3389/fonc.2025.1560437. eCollection 2025. Front Oncol. 2025. PMID: 40416879 Free PMC article.
-
Dual-phase CT for the assessment of acute vascular injuries in high-energy blunt trauma: the imaging findings and management implications.Br J Radiol. 2016;89(1061):20150952. doi: 10.1259/bjr.20150952. Epub 2016 Feb 17. Br J Radiol. 2016. PMID: 26882960 Free PMC article. Review.
-
Clinical Significance and Prognostic Implications of Quantifying Pulmonary Contusion Volume in Patients with Blunt Chest Trauma.Med Sci Monit. 2017 Jul 26;23:3641-3648. doi: 10.12659/msm.902197. Med Sci Monit. 2017. PMID: 28746303 Free PMC article.
-
A possible role of e-FAST in the hemodynamically stable polytrauma patient: results of a single trauma center preliminary restrospective study.J Ultrasound. 2025 Mar;28(1):75-79. doi: 10.1007/s40477-024-00962-0. Epub 2024 Nov 9. J Ultrasound. 2025. PMID: 39521752
References
-
- Mullinix AJ, Foley WD. Multidetector computed tomography and blunt thoracoabdominal trauma. Journal of Computer Assisted Tomography. 2004;28(supplement 1):S20–S27. - PubMed
-
- Miller LA. Chest wall, lung, and pleural space trauma. Radiologic Clinics of North America. 2006;44(2):213–224. - PubMed
-
- Scaglione M, Pinto A, Pedrosa I, Sparano A, Romano L. Multi-detector row computed tomography and blunt chest trauma. European Journal of Radiology. 2008;65(3):377–388. - PubMed
-
- Chardoli M, Hasan-Ghaliaee T, Akbari H, Rahimi-Movaghar V. Accuracy of chest radiography versus chest computed tomography in hemodynamically stable patients with blunt chest trauma. Chinese Journal of Traumatology. 2013;16(6):351–354. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
